DYSENTERY, BERI BERI, MALARIA
‘speedo speedo’
The misery POWs faced: during torrential rain – marching through mud, feet deep, without boots, without clothing to camps 30, 40 or 100 kilometres away or to work sites – unless you are really ill and cannot walk, you may have beri beri, malaria, dysentery or all three! But they don’t count when the Japanese need numbers.
Guards would march into the hospital tent and drag away any number of POWs to fulfil the numbers demanded by the Japanese engineers for the daily work.
DYSENTERY
What is dysentery?
‘acute Diarrhoea, that is passing motions or should I truthfully say blood, 30 to 50 times a day.’
Dysentery is essentially diarrhoea so violent it causes bleeding and death.
67% of all deaths at Tamarkan in 1943 were from bacillary dysentery.
It was one of the leading causes of death in Australian soldiers captured by the Imperial Japanese Army WW2.
Malaria and dysentery were especially common, with most POWs experiencing several attacks each year. Many POWs would suffer both dysentery and malaria at the same time. Dysentery and diarrhoea caused more than a third of prisoner-of-war deaths. Only critically ill were able to rest.
The continuous passing of stools caused dehydration and drained them of vitamins essential to their survival.
As told to Tim Bowden ‘Prisoners of War – Australians Under Nippon’ – The ABC series………………..
‘Toilet hygiene was the single most effective way to prevent cholera. Our doctor, Captain Millard, pulled no punches.
‘If you don’t make it to the latrine, you will infect some of your mates and they will surely die as a result of your carelessness and stupidity. If you get caught short on your mission you are the same as a murderer!’
Following instructions, we dug a new, very deep trench and placed four strong timber planks across it. We then cleared a pathway through the jungle scrub so that the latrine could be quickly reached by those in urgent need.’
‘In the never-ending rain the trench quickly half-filled with water and so to add to our lot, the area rapidly became muddy and the wooden planks precariously slippery. It was always a race against time. There were times when a man slipped,over balanced and fell into its murky depths.’

Konyu, Thailand. c. July 1943.`Dysentery Block’ of makeshift hospital set up in tents at H Force prisoner of war (POW) camp at Konyu 2 (later known as Malayan Hamlet), on the Burma-Thailand railway. H Force was a composite group of approximately 3000 British and 600 Australians. Their headquarters was set up at Tampie (*147 kilometres) and they were spread over a stretch of railway between Tonihan (*139 kilometres) and Hintok (155 kilometres), with the Australians at Konyu 2 (K2) (*152 kilometres). *Distances measured as north of Nong Pladuk (also known as Non Pladuk). H Force did not belong to the Thailand POW Administration, but was on loan from the Malaya POW Administration based in Changi. This problem of remote control caused enormous problems for its POW work force, which lost almost 28 percent of its members, including 179 Australians. The photograph is number 10 in a series marketed by the Far East Picture Company and originating from material used in the Rabaul War Crimes Trials. Original caption reads `10 – Dysentery Block, Kanya’. (Donor H. Clarke). With acknowledgement and thanks to AWM.
Can you imagine yourself as a POW ill with dysentery?
What would the pain be like? How would you feel with faeces all over and about you, lying beside another sick POW? Would you care if you lived or died?
Thinking about dysentery today, i.e. right now, I believe we immediately feel embarrassment. That is until we close our eyes and really imagine how you would cope. Remembering many of those around you are ill too!
Would we really care?
Please read the Australian Defence Force
Journal of Australian Military and Veteran’s Health
Volume 32 Number 3 – July 2024
DYSENTERY is associated with overcrowding, poor hygiene and warm climates. It is highly contagious and can be spread by just a touch.
There was extreme overcrowding in POW camps, with men restricted to the small area of allocated space for sleeping. Conditions were far worse during transportation on trains and ships (Hell ships to Japan and 3-4 day sailing between Java, Sumatra and Burma) and 4-5 day train trips in overcrowded trucks to Burma-Thai Railway.
However the POWs suffering malnutrition and exhaustion after years of incarceration were hardly able to fight off disease.
The folllowing are just some of the challenges awaiting Work Parties at ‘new’ campsites, (for many POWs they would have worked all day at the last Camp, packed up and walked all night and arrived at the new location and be ordered to work:
work party would have to construct a camp
remove the bodies of Romushas who died of cholera
water needed boiling before drinking –
latrines required construction
roofs and walls of existing accommodation repaired
existing camp sites flooded with mud & often faeces during rains
set up new kitchens and hospital wards
Below: POWs had to stand for hours every morning and evening at parades to be counted and for work parties. Imagine being ill, say with dysentery, you probably would have preferred death rather than try to stand while Japanese guards counted the number of POWs over and over again. Which they did often.
Were there enough men for today’s work party?
How many men did the engineers demand?

Above: POW on ground has beri beri is unable to stand, others have bandaged leg ulcers, POW with blanket around shoulders probably has malaria, how many have other illnesses, there are No boots and few clothes – but it is ‘off you to work you go’
-
Beriberi: A thiamine (vitamin B1) deficiency, associated with polished rice consumption.
The Burma-Thai Railway Doctors were excessive at times about hygiene, drinking water and latrines in POW Camps – far more than the British or Dutch. But it saved many lives.
Dysentery is commonly spread by dirty water or food being contaminated with human waste. With diarrhoea comes the threat of dehydration. Loss of water and electrolytes including sodium, chloride, potassium and bicarbonate are lost through liquid stools, vomit, sweat, urine and breathing.
The large Camp Hospitals had dedicated Dysentery (tented) wards.
Amoebic dysentery could be treated with emetine (acquired by Camp doctors usually obtained through Black Market) as there were no official medical supplies for POW Camps. Amoebic dysentery was considered to be more of a chronic condition which lingers and is debilitating.
At Thamby POW Camp in Burma there were 4 deaths of 2/4th men – three died of dysentery and at least 4 deaths of 2/4th men at Khonkan Hospital Camp.
A dysentery register was compiled at Changi.
Please read Australian ‘F’ Force M.O. Dr. Peter Hendry’s views on beri beri
Below: this information is from British Hospitals.
ACUTE BACILLARY DYSENTERY – without treatment a patient lasts only about two days.
https://theses.gla.ac.uk/79671/1/13855707.pdf
DYSENTERY AMONG PRISONERS OP WAR: SINGAPORE 1942-45.
A Thesis for the Degree of M.D.
by Kenneth C. Hutchin, M.B., Ch.B.
Glasgow University.
The largest epidemic of acute bacillary dysentery to occur in the Singapore P.O.W. Camps was the initial outbreak. The Dysentery Wing of the hospital was opened on 11th March, 1942. Two days later the total number of in-patients was 550* The number rose to 800 during the next two weeks and remained at that level for two months, after which the total gradually fell. Prom June to August the total was between four and five hundred. During the first five months 10,000 were admitted to the Wing: the deaths numbered about 120 and the chronic cases 100.
At the beginning of September the Selarang Episode caused a sharp rise in the number of cases of acute bacillary dysentery. The record total of 830 patients in the Dysentery Wing was then reached. This epidemic was not sustained to the same extent as the previous one and by mid November there were only 290 cases in the Wing including 30 amoebics and 90 chronic bacillaries. At the end of 1942 parties began to arrive from Java, and in these: many already dangerously ill with bacillary dysentery on arrival. This caused a fresh epidemic in Singapore during which the largest number of cases in hospital was between 400 and 500. The total number of cases admitted in 1942 was 15,000 and the deaths numbered 245.
During the first half of 1943 the average number of cases in the Dysentery Wing was 200 – When the hospital moved to Selarang in August 1943 there were only 140 cases of dysentery, including amoebics and chronic bacillary cases- At that time acute bacillary dysentery was only occurring as a sporadic disease – only one or two cases a week being admitted In December 1943 about 100 extremely severe dysentery cases of all types arrived from the Burma-Siam Railway working parties.
During the first half of 1944 the total gradually fell and only 40 amoebic cases and 40 chronic bacillary cases were in the hospital when it moved to Kranji at the end of May 1944 From then until September 1945 most of the acute bacillary cases were dealt with in Camp Hospitals at the various Working Camps.
At the Main Hospital in Kranji the number of acute bacillary cases in hospital at one time averaged about ten during that period. All these figures exclude Australian cases, as these cases, apart from those referred to the Sigmoidoscopy Clinic for an opinion, were always treated in a separate Australian Wing. The severity of the cases in the early epidemic of bacillary dysentery was extremely variable. All types from ambulant cases having a few loose stools daily to choleretic / cases in which death occurred in two to four days were seen. It was not possible to estimate the incubation period as the entire community was in more or less constant contact with infection from some source.
-00-
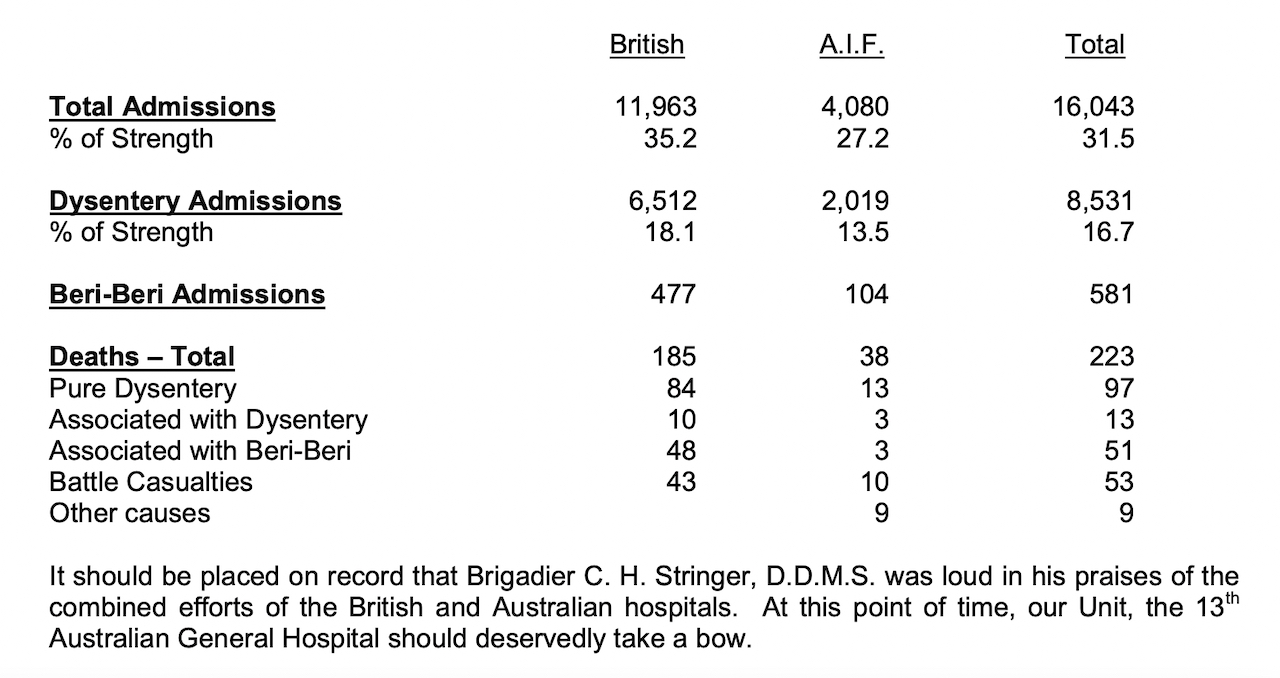
The above figures have been collated up until May 1942. The dysentery patients far outnumber all others. This graph has been taken from history of 13th AGH.
PATIENTS FROM JAVA
On October 11th, 1942, a group of prisoners, containing 362 Australians led by Major Robertson, 2/6 Field Company, sailed from Java to Singapore. On arrival many of these men were admitted to hospital.
Four Officers, 14 N.C.Os and 85 privates, mainly from 2/3rd Reserve motor transport, 2/2nd Pioneers, 2/6 Field Coy, Royal Australian Navy and 2/40th battalion were listed on the nominal roll of No. 3 and No. 4 Java parties presently
in hospital.
These men needed attention for malnutrition, dysentery, malaria and beri-beri. The whole Java Force left for Burma on 9th January, 1943 in much better shape than when they arrived at Changi.
What is the difference between amoebic dysentery and bacillary dysentery?
They have different causes.
There are two main types of dysentery: amoebiasis and bacillary dysentery (without medication the patient dies within two days).
Parasites cause amoebiasis, including E. histolytica, B. coli and strongyloidiasis. Bacteria cause bacillary dysentery, including Shigella, Salmonella, Campylobacter and E. coli.
2/4th Deaths:
22 Dysentery
8 Dysentery & Malaria
19 Dysentery & other illnesses.
Of interest, there were 53 deaths from Malaria and another 10 from Malaria in combination with other illness/s.
This includes numerous deaths at Sandakan and on the track to Ranau where Japanese guards would diligently write ‘Malaria’ as cause of death whether it was so or not.
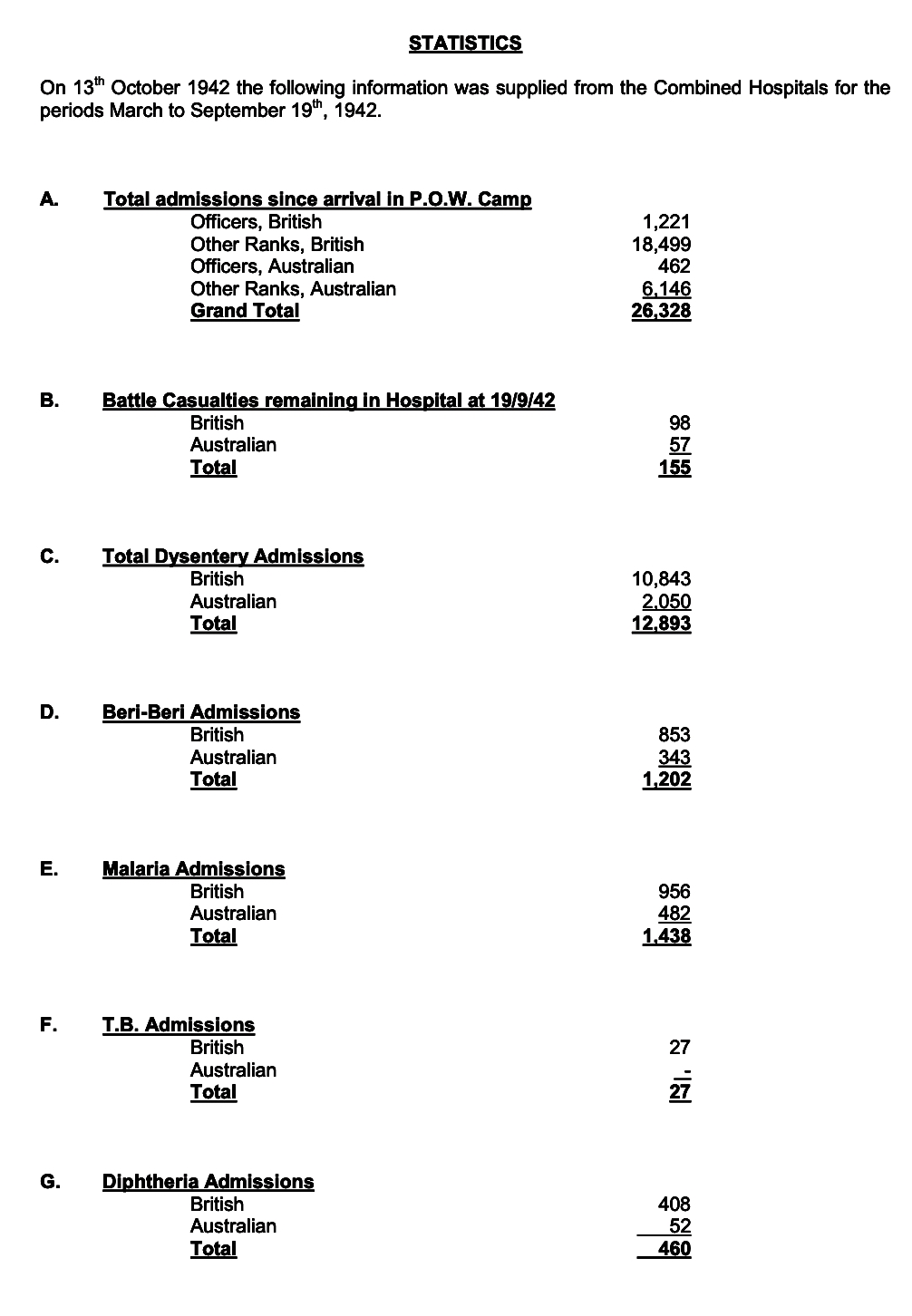
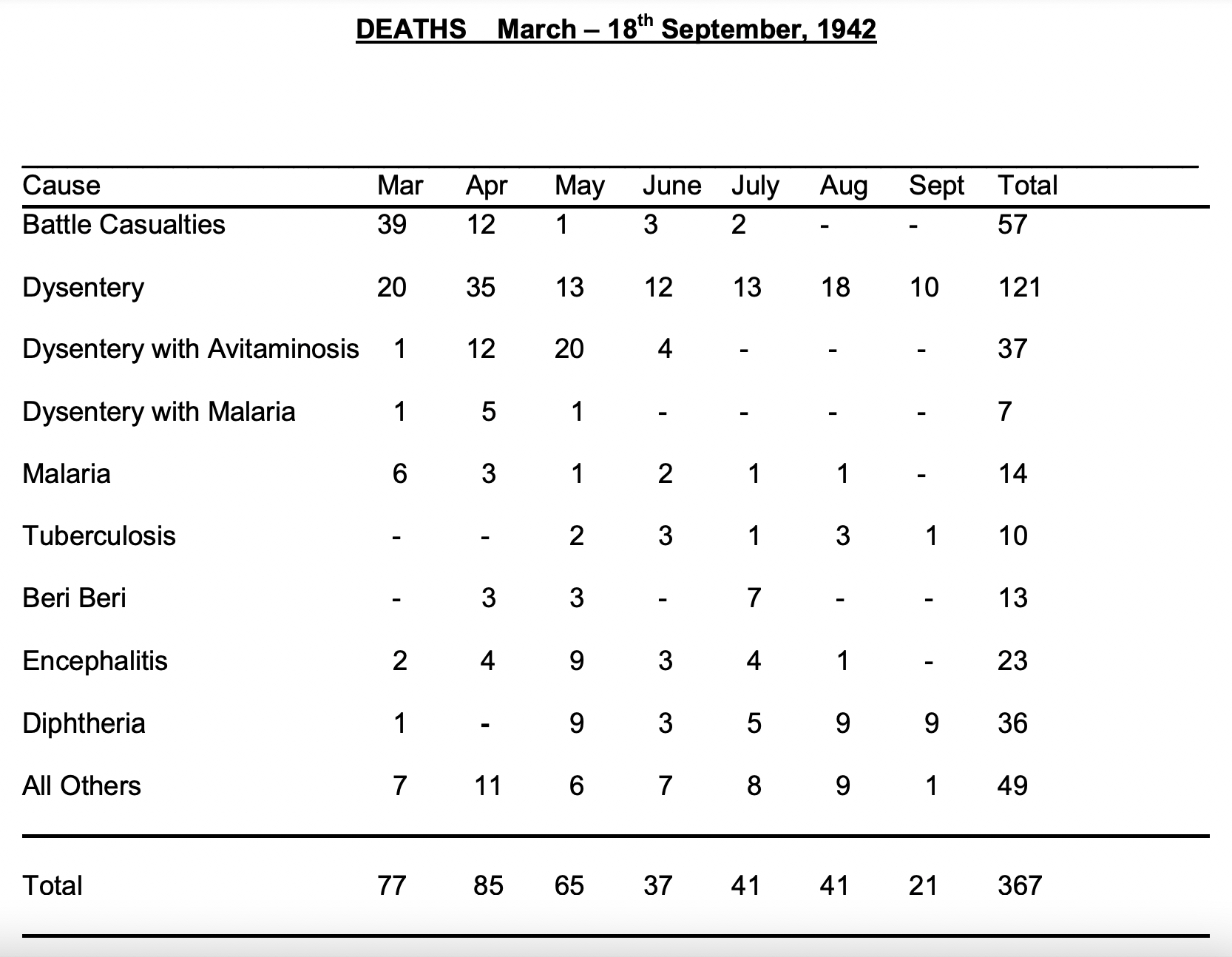
The above figures are from history of 13th AGH.
An injection of Emetine as experienced by the great “Weary” Dunlop.
Extracts from “The War Diaries of Weary Dunlop”, Sir Edward Dunlop describes his experience of suffering from amoebic dysentery at Hintok in Thailand.
“25 May 1943 ….bang, down I go with dysentery, really quite severe. Trying to carry on and have not completely reduced my diet to fluids but have begun M. & B. 693 4g in about 10 hours.
28 May 1943 I am properly ill today with fever and nausea and severe abdominal pain, aching back and weakness. Dysentery intermittently which means slushing outside in the pouring rain and mud….I am eating nothing, fluids just a bit, M. & B. 693 continued 2-3 times a day. I have a hunch that I have really got amoebic dysentery and have had it for some time.
29 May 1943 Pouring rain and wet. I am feeling wretchedly ill….just able to take a little sugared drink. Continuing on M. & B. 693 one four-hourly with no effect.
30 May 1943. Still feeling very sick. Dysentery only slightly less. No lessening in blood and mucus….I am increasingly convinced my affliction amoebic dysentery…
31 May 1943 I am still a cot case, eating almost nothing…
1 June 1943 I took the plunge today and injected myself with emetine hydrochloric grains 1 *
* I collapsed under a tree going to the interminable benjo ( trip to the latrine)
The vultures gathered on the branches above, ignoring my feeble fist-shaking.
There arrived from nowhere Capt. “Legs” Lee RAMC, who felt my pulse and said he would give me some emetine.
I said: ‘Rot – how much emetine have you got?’.
He said ‘I have six grains and you will have half.’
I said ‘No way – you will need all that yourself.’
He gallantly over-rode me and prepared the injection, dissolving the tablets on a spoon.
The following day I was sufficiently improved to throw stones at the vultures!”
M & B 693 Tablets

Clear glass bottle, corked, containing original laboratory sample of “M and B 693” or sulphapyridine, small quantity of yellowish white powder produced by May and Baker of Dagenham, bottle inserted in black wooden mount, English, 1930-1938
M & B 693 was one of the first generation of sulphonamide antibiotics, pro-duced for the first time in 1938. The first chemical cure for pneumonia, it was hailed as a wonder drug. M & B 693 could also prevent the growth of the blood-poisoning bacteria in wounds and was used to protect against gan-grene. It could either be taken in tablet form or the powder could be placed in wounds. It was used so widely during the Second World War that May & Baker had difficulty keeping up with demand. It was later largely superseded by penicillin and sulphonamides.
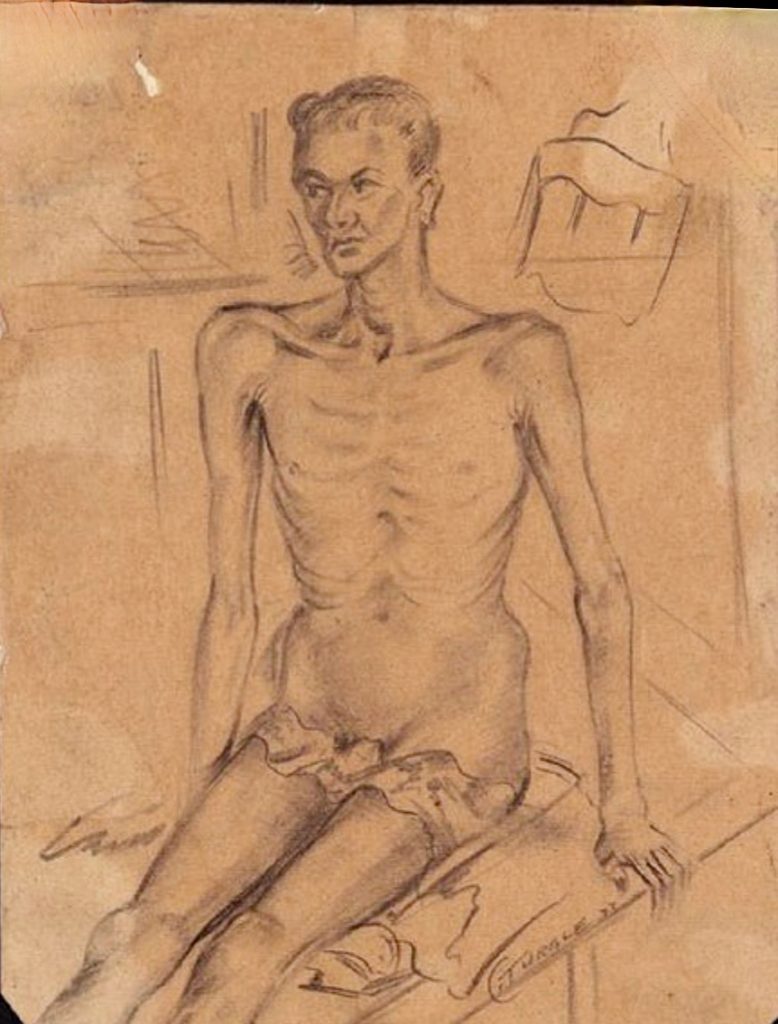
Above: Dysentery patient 1943 Burma. (we acknowledge and thank IWM)

Above: A Confronting photo of POWs of ‘F’ Force with dysentery on their train trip from Singapore to Thailand 1943. It was similar for every POW entrained to Thailand to work.

Above: We wish to acknowledge IWM for above dipiction of a dysentery ward.
Did you know dysentery has played significant roles in Australian military history?
Epidemic dysentery occurred on the Gallipoli Peninsula in 1915 – soldiers were crowded into unhygienic situations for days at a time, there was no water and the rocky soil prevented normal latrine construction. It was a factor in consideration to leave the peninsula.
In Palestine 1918, Australians suffered dysentery in the hot Jordan Valley.
Twenty per cent of autopsies performed at No. 3 Australia General Hospital in Egypt WW1 showed amoeba. Most deaths were either acute infections driven by the Shiga bacterial toxin or chronic infections resulting in malnutrition and debilitation.
WW2 in New Guinea was a prime area for dysentery as well as Queensland and N.T.
There was an outbreak of dysentery for some of the Australian soldiers in Vietnam.
Dysentery through History
During the 1700s and 1800s dysentery disease caused endless deaths throughout Europe.
Diarrheal diseases are among the most common causes of death, especially in children in developing countries. In 2019 around 1.5 million people died from diarrheal diseases.
Malaria on Burma- Thai Railway

In his memoirs, Stanley P. Pavillard, a POW medical officer in the No.4 Camp, states that
“The worst of the acute and dangerous diseases which we were faced with, apart from cholera, was malignant tertian malaria with its cerebral complications.”
Almost everyone on the railway contracted malaria: in memoirs of ex-POWs and former Japanese servicemen, malaria is always mentioned as a disease that the authors suffered from. In most cases, the disease was ʻbenign tertianʼ malaria caused by Plasmodium vivax. However, according to Gill, in remote camps in the jungle, up to one-third of cases were falciparum malaria caused by Plasmodium falciparum, which was malignant and associated with complications, including cerebral malaria.
Pavillard described cerebral malaria patients as follows:
“Patients were being brought in with temperatures of 105°to 107°, and unless the proper diagnosis was made and the proper treatment given at once, the patient would sink into delirium and then into a coma, and his temperature would rise to 110°: after this there was no hope of recovery as his brain was literally cooked. The important thing therefore was to keep the temperature down.”
Pavillard would then slowly inject quinine well diluted in saline into the patients’ veins, although it could lead to sudden heart failure. It was the only life-saving technique they had. Quinine is usually used to treat uncomplicated malaria, not severe forms of the disease. Nevertheless, the only medicine that the IJA could provide to treat malaria was quinine, and a sufficient amount was available.
In his report, Tagami states that: Even the Japanese forces in this [Thai-Burma border] area, when outbreaks of malaria occurred, would have been without the ability to carry out operations but for the fact that we had a considerable stock of quinine.
Thus, the POWs could obtain the medicine sufficiently. Also POW medical officers could get more quinine from the Japanese by padding the number of malaria patients. For instance, Hardie, a medical officer in the No.2 Camp, states in a note for his diary that, at first, in view of the inadequacy of the supply of quinine, he was compelled to inflate the number of malaria patients. However, in the entry on 7 July 1943, Hardie states that they were getting enough quinine to treat active cases.
Pavillard also padded the number of malaria patients and obtained more quinine than he needed. Eventually, the ʻemergency reserveʼ of quinine was exchanged with a cow owned by a local Thai resident.
Pavillard adds that “It was impossible to cope with malaria and its complications properly.” Besides the insufficiency of malaria preventive measures, there was a problem among the POWs. Even after a sufficient amount of quinine became available, many POWs refused to take the medicine either for prevention or cure. Pavillard often found the pills, supposed to have taken, hidden under their pillows after they had died. Presumably, the POWs refused the medication for its adverse effects. Therefore, prevention became still more essential. Accordingly, mosquito-nets and blankets became precious items, and thefts became frequent in the POW camps. Baynes recollects in his memoirs as follows:
There was unfortunately a lot of thieving from comrades going on in Chunkai camp. […] Blankets, most valuable of all the captiveʼs possessions, were stolen and sold to the Thais. With no protection from the malaria-carrying mosquito many must have died solely because of these camp thieves. Even the medical hut was broken into and our scanty supply of medicines robbed for private gain. Some became so wealthy that they were able to bribe those in charge to let them stay in camp as sick men, while the really sick were forced out to work.
There was friction among officer POWs in the No.2 Camp regarding anti-malaria activities such as oiling mosquitoes’ breeding grounds. When Hardie formed an anti-malaria working party comprised of officers, some officers worked hard, but others were reluctant, saying that officers should not do the work. Moreover, in his diary, Hardie criticises Williamson, the No.2 Camp Commander, for his uncooperative attitude towards the anti malaria party. Hardie said that:
apparently the Japs are trying to get more officers out working on the railway and it looks as if Colonel Williamson, anxious as ever to comply, was trying to put the blame on me for the necessity of turning the anti-malaria party officers on to railway work.
So, not only mosquitos but also enemies and comrades were the factors that made malaria prevalent among the POWs!
We wish to ackowledge the above Malaria information has been taken from
Constructing the Burma-Thailand Railway: The War Crimes Trials and the Shaping of an Episode of WWII – by Kazunori Hashimoto. Thesis submitted for the degree of PhD YEAR 2022