‘H’ FORCE GROUP
The overall commander for H Force was Lt-Col H.R. Humphries while Lt-Col R.F. Oakes commanded the Australian contingent of the force numbering about 600.
H Force totalled more than 3,000 POWs.
H Force numbering 3270 POWs left Singapore in 6 train lots during the period 5th to 17th May 1943. Consisting of 1141 British, 670 Australians, 588 Dutch, 26 Americans, Malay Volunteers and Indians made up the rest. A unique feature of H Force was an Officers Party made up of 260 Officers who worked as labourers. Like F Force they remained under the control of Singapore Command and suffered accordingly.
This work Force departed Singapore by train morning 8 May 1943, arriving Non Pladuk four days later on 12 May.
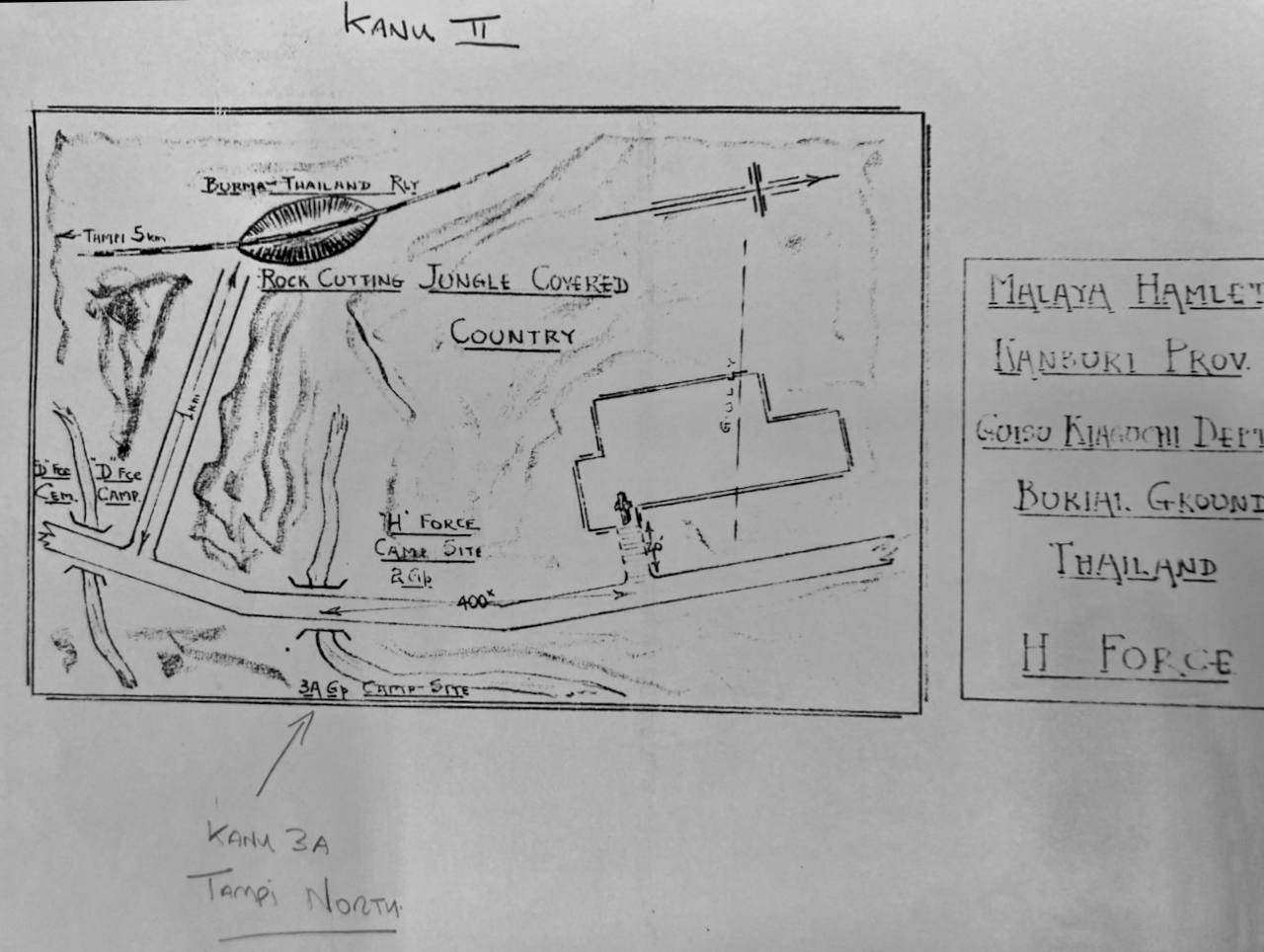
Initially this group went to Tonchan Camp 139 Kilometres north of Non Pluduc. The Australians under Lt Colonel Oakes with Major Saggers 2/IC went to Konyu Camp 2 and worked on the Hellfire Pass Cutting, also the Three Tier Bridge, which took a deadly toll of the men. In August 1943 100 Australians were selected and force marched to Konkoita to join F Force on a cutting that was running behind time.
Major Bert Saggers from 2/4th was second in command to Lt- Col Oakes and in charge of the group’s pay and records.
Australian Medical Officers were Majors Ernie Marsden and Major Kevin Fagan.
Unfortunately, most of the men were older or not in the best of health. This resulted in a high death rate and worse still, limited work quotas for the Japanese and meant sick POWs often went to work.
While exact figures vary, sources indicate a total around 850 died in H Force, which included approximately 600 Australians. This represented a death rate of about 27.37% – 43% for the force, with conditions such as prior illness, malnutrition, and poor treatment contributing to the high .
From Non Pladuk the men marched to nearby Konma Transit Camp, staying overnight. The following night they began their march to Malayan Hamlet – 170 km march to their camp site would take 5 days.
The following day 13 May 1943, this group marched out of Konma transit camp at 2300 hours, arriving at their first rest camp at 1000 hours the next day. ‘H’ Force followed in the steps of ‘F’ Force to Kanchanaburi heading for Malayan Hamlet/Kanu II.
(POWs were mostly marched at night to avoid intense day heat – night marches then subjected men to other horrors such as marching in total darkness – dense tall jungle growth blocked any light shown from stars and moon which made the tracks difficult to find and to follow. Men injured themselves slipping off the tracks off into growth, down slopes, etc. Many men had poor quality footwear, maybe none and tripped on stumps, rocks injuring themselves). At Kanchanaburi the POWs slept while local Thais stole whatever they could escape with! Marching on an average of 15 miles per night they covered a distance of 90 miles by 0400 hours on 21 May to arrive Konyu III. The final trek of about 4 miles to Malayan Hamlet took 3 hours through dense and rugged terrain.
Although they started out as an Australian workforce, ‘H’ Force Group 3 had collected along their journey, 114 British and some POWs from Java. On 30 May 1943 an additional 98 stragglers marched in to join them. There would be 500 Australians, 200 British and some Americans at Malayan Hamlet (Konyu 2).
106 British and 111 Australians would die at this camp.
Malay Hamlet was approximately 450 yards east of Hellfire Pass Cutting and to the north of ‘D’ Force S Battalion’s Camp Konyu II. The road from Tarsau passed to the right side of both Konyu II and Malayan Hamlet Camps.
They arrived exhausted to find there was no established camp – the location was a small area of uncleared and sloping ground. They immediately pitched 20-23 tents – rotting and leaking to each sleep 28 men – although with the shifts this number were never present at one time. Cookhouses and latrines had to be built.
And worse it was beginning of monsoon season.
‘Almost immediately the monsoon rains began, pouring down day after day, until the country became like a wet sponge. In our confined area, and on the track outside which carried the traffic, mud was often knee deep—filthy, oozing mud which stuck to everything like glue. We made a few poor bamboo tracks in the camp area, but it was difficult to provide labour to maintain them. I doubt if any of us or our belongings were dry during the first month in that camp.’ – Lt-Col R.F. Oakes From Anzac Portal
Water carried from a nearby stream and had to be boiled.
The workforce was split into four shifts with each shift consisting of 100 men.
Two shifts worked daylight hours and two shifts worked the night. Immediately ‘H’ Force knew they did not have sufficient fit men to cover these shifts. It was of no consequence to Japanese – they demanded sick make up the required force.
During the first months food and supplies were limited and erratic. First and most significantly while in Thailand, H and F Force remained under the control of the remote Imperial Japanese Army Malay administration. In other words H and F Force were not allowed to access supplies from Japanese occupied Thailand. They had to wait on supplies from Japanese occupied Malaya!
Most of their supplies never arrived.
The ration level for ‘H’ Force was well below subsistence level. Combined with poor leadership, violence from Japanese/Korean guards, monsoonal weather and ‘speedo’ no doubt increased the death rate for Australian POWs.
The Thai administration of Imperial Japanese Army (Kanchanaburi was main HQ) controlled the other work forces, such as ‘D’ Force in this area of rail construction.
Food could be bought from Thai traders who had barged food supplies by river to Konyu River Camp. This was several kilometres away from Malay Hamlet and carrying parties had to be drawn from the same men working on the rail link (as Japanese engineers required their full quota of working men).
Exhausted POWs would arrive back from working as long as 12 hours or more and have to walk kilometres to the river and back with supplies!
It did not occur to the officers (or perhaps it did) that they could have in fact organised themselves to go to the river for supplies as they were not required to work.
When the first confrontation arose with the Japanese leadership over the men’s work conditions, Oakes was quick to step in. He also walked away just as quickly and the Japanese leader knew he would have little opposition. Oakes clearly showed a preference for his own self-interests. The men soon lost respect for Oakes and his leadership. An awful prospect for the men.
By default, Doctor Kevin Fagan (please read further https://www.pows-of-japan.net/articles/6.htm) became leader of ‘H’ Force, probably more so of those sick. As chief MO with huge numbers of sick and dying men and well as Camp leader his role became an overwhelming challenge. The men who were not sick quickly formed strong support groups to survive.
Three weeks after their arrival on 16 June the first case of cholera appeared at the Camp – the patient died 6 hours later. The Chief MO Major Kevin Fagan was to work extremely long and difficult hours not only with cholera, but malaria, tropical ulcers, beri beri, etc.
With arrival of cholera two tents were pitched about 165 yards away from the main camp to accommodate patients. There was cholera at Konyu II and Hintok Road Camp.
During the height of the cholera crisis the camp was burying twelve men a day. The death toll within a ten-week period rose to 216. Conditions and the death rate did not improve.
On 25 August 1943 the Malay Hamlet rail link was considered complete and a combined force of 83 Australian POWs from H3 and H6 joined some British POWS to form ‘H’ Force No. 1 Sub-Section – they travelled by train to Konkoita area in a last minute dash to complete the railway in that sector. The selection of this combined Force of 100 POWs was made by Chief Medical Officer with ‘H’ Force, Doctor Kevin Fagan. Many years later Major Fagan said it was the worst thing he had to do – that is to decide the fate of those 100 men of whom were all suffering ill-health and send them to Konkoita to face further work. He dreaded to think what happened to them.
Kevin Fagan was wonderful and dedicated surgeon who saved many lives. Pre-war he had been a senior surgeon at Sydney Royal Hospital and as with all doctor on the Railway – the men he treated praised his work and dedication.
On his return to Singapore Fagan was himself in a state of complete exhaustion and critically ill with cerebral malaria at Sime Road Camp. He was held in such high esteem that half hourly bulletins were issued on his condition – fortunately he recovered.
On 8 September the first evacuations of sick from ‘H’ Force were taken to Kanchanaburi. Over the following days another four parties were evacuated totalling 500 men which left 25 POWs to clean up the campsite area.
On 16 September the rear party who had been working at Tonchan Spring Camp moved to Tampie North Camp to join the other Australians before this last group also moved to Kanchanaburi.
‘H’ Force returned to Singapore at the end of December 1943 when the rail link was completed. Oakes never regained the respect of his men and reported his own version of events to Galleghan at Changi and in his official war diaries.
You may like to read further about Lt-Col Roland Oakes
The above overview of the leadership of Oates is not to be found on AWM – with time this is a widely recognised and accepted opinion by numbers of ‘qualified’ persons who have researched leadership of POWs (and does not include leadership in war-time). This information has been included is because it has been widely researched and it is important that we, more than 75 years later have an opportunity to begin to understand what the POWs of Japan lived through every day, every week and every month they worked on the Burma-Thai Railway, Japan, and Sandakan. Those who were fortunate to return to Changi for the last 18 months of war, agreed it was a relief to be back, ‘it was like being back at home’.
They were safe.
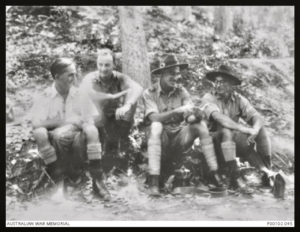
Below: Oakes on Left


Above: Oates on left
Below: Oates seated in centre.
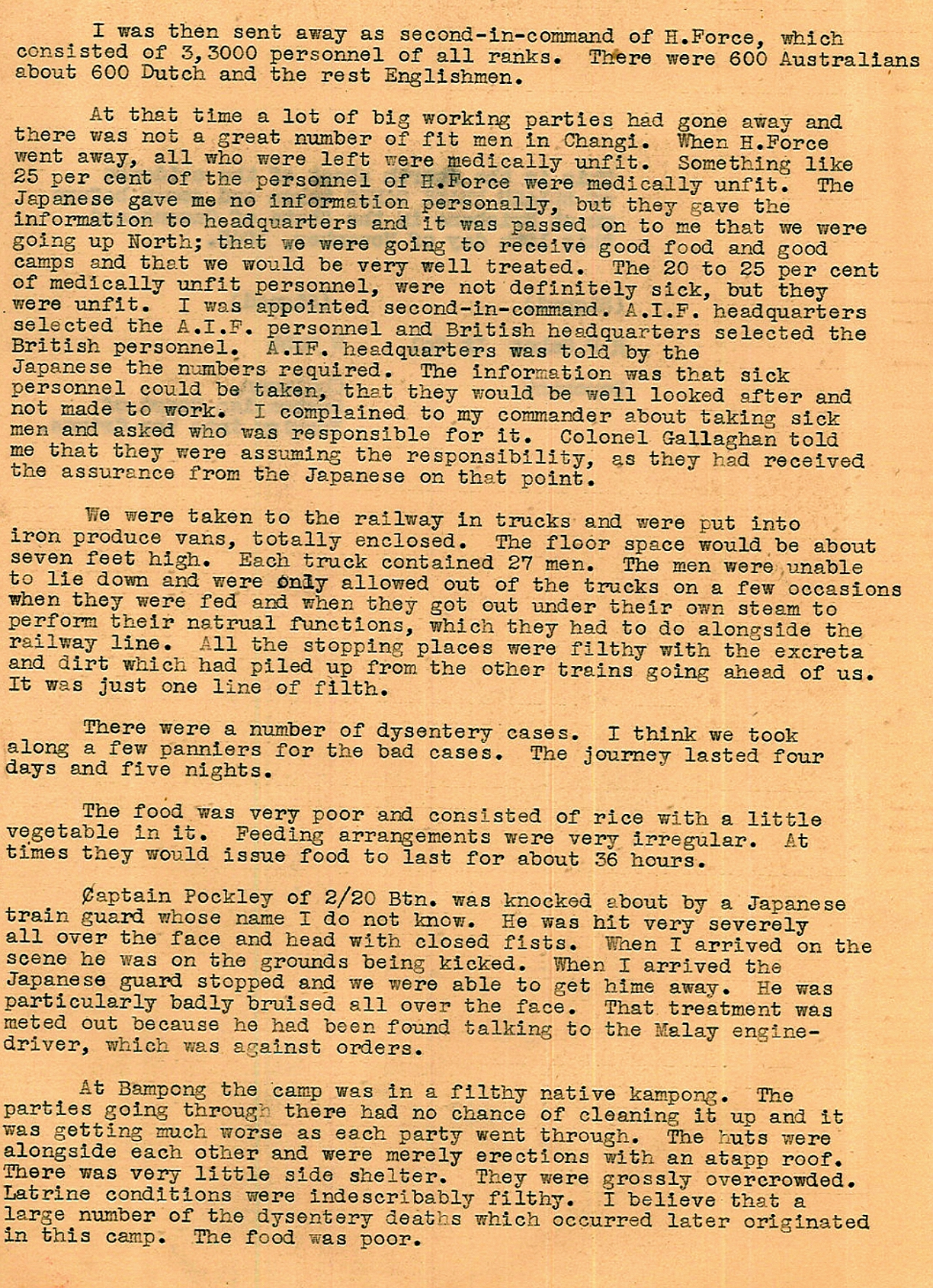
Below: A page of Major Saggers’ notes on ‘H’ Force.
__________

We wish to acknowledge much of the following has been copied from Peter Winstanley’s webpage.
In Katie Meale’s doctoral thesis on ‘Leadership of Australian POWs in World War II’ for the University of Wollongong, she quotes Gunner Russell Braddon in his book The Naked Island writing about Major Kevin Fagan: ‘Not only did he treat any man needing treatment to the best of his ability, he also carried men who fell; he carried the kit of men in danger of falling, and he marched up and down the whole length of the column through its entire progress. If we marched 100 miles through the jungle, Kevin Fagan marched 200. And when, at the end of our night’s trip, we collapsed and slept, he was there to clean blisters, set broken bones and render first aid.’
WITH ‘H’ FORCE, FAGAN WAS KNOWN for his compassionate care. Wonderful surgeon.
Kevin Fagan had an extraordinary gentleness, that made you feel as though you were his only patient.
In the POW camps, examining and consulting hundreds of critically ill men every day, with minimal facilities, performing necessary operations on rough bamboo platforms in the open air of the jungle, he did so with the good humour and courtesy of someone being richly paid for their specialist services.
From the time of his arrival in Thailand, his days were completely occupied with attempting to control a severe epidemic of cholera in men who were suffering from chronic dysentery, malnutrition and tropical ulcers. By the time that H Force was evacuated back to Syme Road in Singapore, he was in a state of physical exhaustion, and was critically ill with cerebral malaria. He suffered fever and delirium for more than a week. Looking back on that period, Bob Goodwin recalls; I can well remember how anxious everyone felt about his illness, and how relieved we all were to hear news of his recovery.
Kevin Fagan returned to Australia to resume specialist surgical practice in Macquarie St. Sydney, with hospital attachments to Lewisham and Royal North Shore Hospitals. He retired from medical practice in 1970 to become a full time grazier, on his sheep property Cooinda, in the Yass District.
Les Cody (in his book Ghosts in Khaki) had this to say:
“Major Kevin Fagan was the chief Medical Officer with the Australian contingent in ‘H’ Force and like his counterparts all up and down the line became another ‘Horatius at the bridge of life’ to the hundreds of prisoners in the Malayan Hamlet camp at Konyu.”
Don Lee (Lt) in his book “A Yarn or Two” said:
“The Camp Medical Officer, Major Kevin Fagan was ordered by the Japs to detail one hundred men to remain and continue working on the railway, while the remainder were to go South, presumably back to Singapore.
Kanu No. 2 was a shocking jungle-camp and in our few months there we had had awful casualties.
In 1987 Major Fagan appeared on a T.V. documentary relating to the Thai-Burma Railway. In an interview he said that the worst thing he had ever had to do was to detail those hundred men, in view of the dreadful state ill-health and sickness existing in the camp. He stated that those men chosen must have hated him and that he had never heard of the fate of a single one of them. I was one of them and we went by rail to Konkoita, about a hundred kilometers away. On arriving at Konkoita, I was detached and sent with an all-Officers Working Party to Konkoita South. The others remained at Konkoita.
Following the documentary, I wrote to Major Fagan, assuring him that I held nothing against him and doubted that any of us did. He was, like all of us, obliged to carry out a very distasteful job. He was a wonderful Doctor and Surgeon and our camp was incredibly lucky to have had his services.
Major Fagan, throughout, at Kanu and all other camps, did a fabulous job. I cannot understand, in view of the wide publicity given to other Doctors, why greater recognition was not accorded to this wonderful and dedicated surgeon. Pre-war he had been Senior Surgeon at Sydney Royal.
In Syme Road Camp Major Fagan took seriously ill. He was held in such high esteem that half-hourly bulletins were issued on his condition. Eventually he recovered.”
Stan Arneil said in his book “One Man’s War”:
“The medical teams were wonderful. Dr. Kevin Fagan operated on my ulcered feet and on Doug’s too. I am not sure how many operations would be considered to be normal in one day in Australia but we believed that Kevin Fagan and his little team performed forty to fifty ulcer operations each day. I am sure that there were other doctors there too but Doctor Fagan’s name was the one we talked about as he was the surgeon who performed all the operations on the group of patients in my hut.”
Extract from MJA Surgical Experiences as a POW
By K. J. Fagan, Sydney
May I begin with a controversial statement? It is this: that the returned prisoner of war is in most cases not only a normal man, except for some temporary physical disability, but one who has had intellectual and emotional experiences which give him a decided advantage over his fellows. He has learned to appreciate the minor pleasures of life. He knows the essentials of existence. He has a high threshold to the pin pricks of ordinary life. He knows man for what he is – his courage, his cowardice, his limitless generosity, his gross selfishness, his nobility and his utter meanness. And if he tends towards cynicism at the discovery of the relation of man’s best qualities to his intragastric tension, he is robbed of all bitterness by the memory of the heights to which he has seen some men rise in spite of starvation, of illness and of every degradation which a malignant enemy could put upon them.
At the relief of Singapore in September 1945, the Press was in the vanguard. My first contact with the outside world was with one of its representatives, who curtly brushed aside all my perhaps incoherent demands for news with the request: “Come on, Major, tell me a horror story.” I did not tell him a horror story, nor do I propose to tell you a horror story: but in a talk on surgical experiences as a prisoner of war, some account of the background is necessary.
Our first surgical task after imprisonment was the care of battle casualties. In Singapore we were fortunate in that for the first few months we had an X-ray plant, plaster, anaesthetics and equipment, so that we were able to treat these casualties secundem artem. Our difficulties were malnutrition and intercurrent infections, particularly dysentery. One frequently had the experience of losing a patient from acute dysentery after months of work at a stage when his injuries were satisfactorily dealt with. A timely shipment of South African Red Cross food saved many of our battle casualties. It enabled us to feed them normally for a long enough period to restore their powers of resistance and healing.
In May 1943, I was detailed as surgeon to a party of 3,500 troops travelling north to Siam to work on a railroad. After a protracted and uncomfortable railway journey to Bampong in southern Thailand, followed by a most arduous march of 120 miles into the jungle, our men were set to work without being allowed time to recover from the journey. They worked for twelve to fifteen hours a day, making a cutting through solid rock with pics, shovels and hand drills. Their rations were grossly deficient in proteins, fats and vitamins, particularly thiamine and the B1 complex. The region was highly malarious; the native population was admitted by its own government to consist of 100% amoebiasis carriers. Very soon our men
were reduced to the status of a malarious, dysenteric, underfed and overworked slave gang. An epidemic of cholera killed 25% of the camp strength in six weeks. With this classical background an epidemic of acute phagedenic ulcer appeared three weeks after our arrival in Thailand. The spontaneous ulcers appeared first as a small vesicle surrounded by an area of redness, induration and tenderness. After twelve to twenty four hours, the vesicle burst, discharging a little sanious material and exposing a sloughing base, which spread with varying rapidity and to a varying depth. In the more severe cases there occurred progressive destruction of skin, subcutaneous tissue, deep fascia, tendon, intermuscular fascia, periosteum and bone. Muscle was relatively immune. The spread of the lesion was accompanied by intense pain and moderate toxaemia. A man with a severe, untreated ulcer presented an appalling spectacle. One saw a pale, wasted man with a flexed knee and a thin strip of intact skin down the calf or outer side of the leg, the rest of the leg being the side of a huge ulcer from which poured offensive, greyish pus; sloughing tenons and fasciae were exposed, the muscles were tunnelled and separated by gaping sinuses, the whole of the tibial shaft was sequestrated.
Conservative treatment was slow and troublesome. It was found that the best treatment was early excision of the necrotic tissue. If one could excise this before the deep fascia was penetrated, cessation of the necrosis, the appearance of healthy granulation tissue and healing, perhaps in the case of larger ulcers with the aid of skin grafts, could be confidently anticipated. Operation in these cases was followed by immediate cessation of pain. Once the deep fascial barrier was penetrated, secondary operations such as excision of necrotic tendons and sequestrectomy were often necessary. In the advanced cases, such as that described above, amputation was the only possible treatment; but the mortality rate was very high. The association of chronic diarrhoea was a particularly lethal factor. However, amputation enabled many of these unfortunate men to die in greater comfort and dignity.
The facilities available for surgery in the Thailand prison camps were not elaborate. My operating theatre, for example, was at first the open air, later a tent fly, and still later, when we returned to the plains at Kamburi, a luxurious affair of palm leaf with a mud floor, but completely fly proofed with American Red Cross mosquito netting. Sterilizing of towels, instruments and dressings was done in a four gallon “dixie” on an open fire outside the operating theatre. Under these conditions, in addition to excisions of ulcers, such operations as appendicectomy, mastoidectomy, craniotomy, “pinning” of the tibia and skin grafting were performed with a minimum of septic complications. This fact was due to the skill and devotion of the theatre orderlies, who fortunately had received their training in better circumstances and earlier in our captivity.
I should like to close with the surgical lessons that I learned as a prisoner of war. The first is that the necessary surgery can be performed in any circumstances, provided fuel and water are available, and provided one has an operating theatre staff adequately trained and accustomed to improvisation. The second is the value of the Steinmann pin in treatment under primitive conditions of fractures of the lower limb. Its simplicity and portability make it invaluable where no plaster, strapping or bandages are available. The third is the value of chloroform as an anaesthetic agent under conditions of tenuous supply lines. It is safe in good hands, and economical. One can carry a large number of “chloroform anaesthetics” on one’s back. The final point is that male medical orderlies can be trained to the safe standards of efficiency and skill in operating theatre technique as women, and that it should not be necessary ever again to expose our women to the danger of captivity at the hands of an Asiatic enemy.
The above was read at a meeting of the New South Wales Branch of the British Medical Association on March 15, 1946.
Source: The Medical Journal of Australia June 1, 1946.
Pp: 775,776
The Australian Medical Association has given approval to reproduce.
Notes collected by Lt. Col. Peter Winstanley OAM RFD JP (E-mail peterwinstanley@bigpond.com ) with assistance from Don Lee
Major Fagin. I first got to know Major Fagin at Siam Road when we returned from the railway to Singapore Island. Now I was just a patient living in the officers quarters. I don’t think I did any medical work. But Kevin Fagin was busy operating there at Siam Road and a man named Austin Best was giving the anaesthetics and he had a technique of conserving ether I suppose it was. I had a small kit of operating tools. Kevin’s, a lot of them, were his Spencer Wells forceps weren’t very good. I know I debated whether to give him mine or not, then I thought, ‘Well look you fool, you goat, you better to stick to it because if you’re sent away you won’t have any’. So I didn’t give it to him. I felt bad about it. I mentioned to him I had these but … so when I got back to Singapore a month or so later I handed it all in. I handed everything I had in so that my conscience was assuaged. But I know Kevin brought back with him a tremendous reputation for what he had done on the railway line. People were full of praise. And when he had a gastrointestinal haemorrhage and he was in a low state in Siam Road you were more interested in knowing how Major Fagin was than what the world news was. It was almost as if part of the camp sort of stopped as it were. He was apparently gravely ill for some days. Anyhow he survived, went back, didn’t see much of him back in Selarang Barracks or in the gaol later. He was a very quiet man, he was loved by everyone. When he had to retire, he had some ill health, then he went down … END OF TAPE TWO – SIDE B START OF TAPE THREE – SIDE A Identification: This is reel four of the interview with Doctor Roy Mills.
Then in October 1990 on our way back driving from Melbourne we telephoned Kevin Fagin and saw him on the property south of Yass. We called, he invited us to have afternoon tea. We had a wonderful chat with him. My wife had started nursing at Prince Henry Hospital in 1937 and Kevin at that time was a RMO there apparently, so they had a good old yak. And then Kevin – the delightful person that he is – confided to her a worry that he’s carried all these years. The superintendent at Prince Henry Hospital, Little Bay, was Cec Walters and I got to know about Cec Walters because Win my wife had been the top nurse in the year but there were a few old battleaxes that made the nurses’ life hell. So in her second year she just handed in her resignation. Doctor Walters called her up and I can remember her description: he always had a little carnation in a button hole. And he said, ‘Look Nurse Plum, what’s all this nonsense?’, and he tore up her resignation and threw it on the floor. So she said, ‘Doctor Walters, you can pick that up’, and she let it stand. Then the other thing about Cec Walters that I remember hearing was that to the consternation of the veterinary surgeons when the famous racehorse [Rogilla] got some trouble with his windpipe – see Cecil loved horses, loved going to the races – the racing fraternity regarded him as better than the vets and they got him to operate on the windpipe of Rogilla, this famous racehorse. So throughout the medical world and the veterinary world Cec Walters’ name was known as the surgeon who operated on Rogilla’s windpipe but not as the superintendent of Prince Henry Hospital. So he was apparently an unusual man and the story I’m coming to was that there was some very important, rather famous ball – charity ball – at which the medical profession was expected to attend. And Cec Walters’ wife was longing to go but Cecil wouldn’t take her. So she persuaded this very fine young RMO, Doctor Kevin Fagin, would he go to the ball. So Kevin accepted her invitation but didn’t realise that he was to take the superintendent’s wife to the ball. He thought he was going to accompany the two. But he was committed now and it worried him at the time that there he was taking the superintendent’s wife to the ball. And he said it’s worried him ever since. Oh dear we laughed. Oh we laughed and we had a lovely cup of tea. It’s sad that his eyesight has been troubled so. He has a restricted driving licence and he can drive five miles along the road near his property so that he can help muster sheep and do things in a truck. He had a little bit of trouble driving the truck but I would never go to Canberra again without going to see Kevin Fagin. He’s just one of these wonderful men and so modest; so very modest. He certainly would like you to visit him again. Of course I would. I wouldn’t dream not. But we’ll have to drive to Canberra.
Dr Roy Mills said of Kevin Fagan’ He’s just one of these wonderful men and so modest; so very modest.’
Doctors we well aware of those officers who failed their men.
Documented records and personal diaries from Australian medical officers in World War II indicate that they were acutely aware of leadership failures among some Australian officers in Singapore and Thailand.
While the narrative of POW life often highlights “mateship” and heroism, medical personnel frequently clashed with officers over the treatment of men and internal camp politics.
Key Observations by Medical Officers
-
Authority Clashes: Medical officers often functioned as de facto leaders because they were the primary defenders of the sick. This led to friction with combatant officers who insisted on traditional military hierarchies. For instance, Edward “Weary” Dunlop famously clashed with Lt. Colonel Frederick “Black Jack” Galleghan in Changi over Dunlop’s authority as a “non-combatant” commander.
-
Selfishness vs. Sacrifice: Diaries from doctors like Dunlop and Rowley Richards record instances of officers prioritizing their own comforts. Dunlop’s diaries noted tensions where officers (including some Allied Dutch and British) were seen seizing furniture or resources for themselves while the general rank-and-file suffered.
-
Maintenance of Petty Discipline:
Some officers were criticized by medical staff for trying to maintain strict, often irrelevant military discipline (such as saluting or formal parades) in horrific conditions where such energy would have been better spent on survival or hygiene.
-
The Burden of “Non-Useful” Men: In many camps, medical officers had to battle their own commanders to keep “no-hopers” or the severely ill from being sent to work details, as some officers were more compliant with Japanese work quotas than doctors felt was humane.
The Role of Doctors as True Leaders
Because many traditional officers were perceived as ineffective or overly rigid, the doctors often assumed the role of moral and physical protectors.
-
Innovative Survival: Doctors like Rowley Richards and Albert Coates relied on “bushies” and resourceful soldiers to build medical equipment rather than relying on formal officer structures.
-
Standing Up to Captors: While some officers were hesitant to provoke the Japanese, doctors like Dunlop frequently risked their lives to physically stand between Japanese guards and sick prisoners, earning them more respect from the men than many traditional commanding officers. (Dunlop was very tall and had been a boxer – I am positive this gave him confidence when dealing with the Japanese)