WHAT DID SCIENCE LEARN FROM NEARLY 4 YEARS OF JAPANESE POW LIFE?
The men suffered numerous tropical illnesses – never before known to them. The hard-working and dedicated Doctors, particularly on the Burma-Thai Railway also learned of illnesses previously unknown to them – learning on the job one may say.
These diseases were the foremost cause of death on the Burma-Thailand railway. Almost every POW fell ill as a result of excessive work, malnutrition, poor food and Japan’s refusal to provide anything but minimal medical supplies.
The men often suffered from more than one disease at any time. Men who would have been considered seriously ill in former civilian working days, had to continue working and working long days with minimal food and water. Only the critically ill were permitted to rest and then received half rations!
It was different in Changi – the medical fraternity was able to pool all their resources – which was not sufficient. They were forced to implement, use their initiative, bribery on the outside and really dig deep.
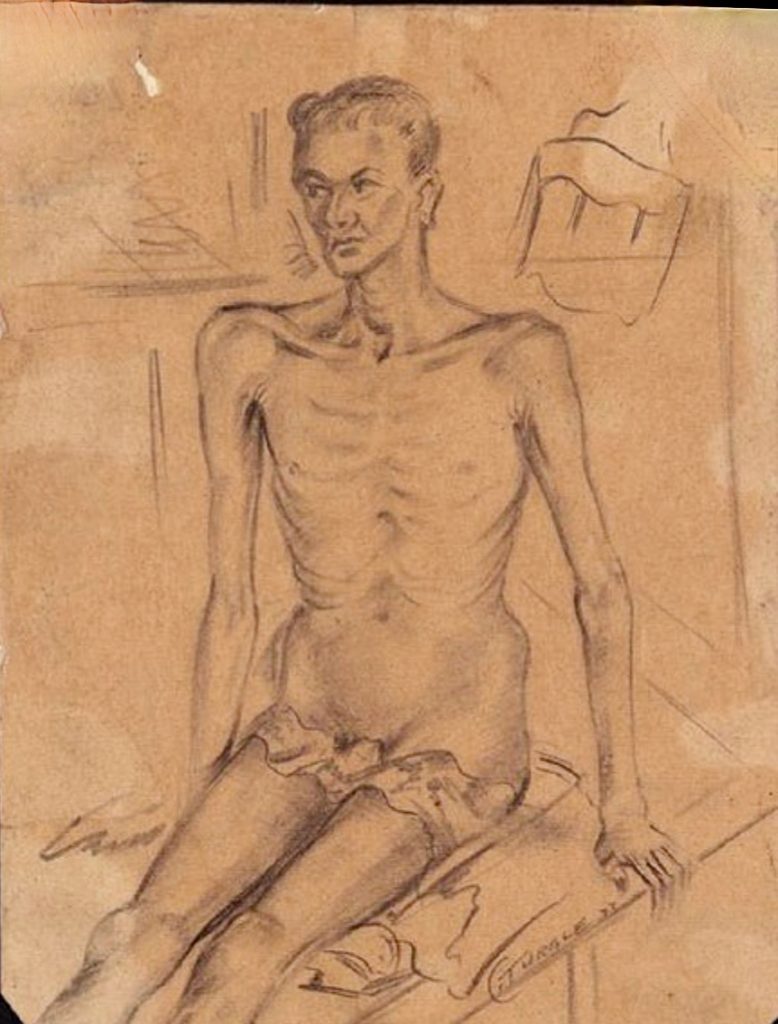
The POW diet, consisting of mostly of small servings of low grade rice failed to supply Vitamins A, B1 and B2 complex, Vitamin C and D, proteins, fats and calcium.
At Changi it became almost immediately evident the men were lacking ‘B’ Complex vitamins resulting ‘Happy feet’, in beri beri and skin dermatitis efffecting every part of the body, including the scrotum, followed by eye conditions such as ulcers of the cornea and amblyopia resulting in young men going terrifyingly and slowly blind. Tragically so many POWs permanently lost a percentage of their eyesight, or worse, became blind.
The Japanese ignored all requests to alter the POW diet. They also refused the surgeons’ request for pure alcohol essential for the sterilisation of medical equipment in the hospital.
AIF medical staff knew they would have produce their own alcohol – and so they did. Part of this alcohol was given to the men going blind. The affects were almost immediate.
Riboflavin available from fresh fruits and vegetables was essential the POW’s eyesight and nervous systems.
On the Railway line – doctors faced a new terror!
Ulcers so deep one could see the bone of the limb. Ulcerated limbs often required amputation resulting in death. Those who survived required the means to walk again.
“The Civil War’s surplus of amputations, gunshot wounds, and mental breakdowns gave America’s newly professionalizing neurologists plenty of patients and opportunity to investigate the intricacies of the nervous system …………”
“Soldiers during World War I came down with “shell shock,” “soldier’s heart,” and “effort syndrome”—all neurasthenia-esque conditions that had no obvious organic cause but needed to be distinguished from the general neurasthenia commonly associated with overworked businessmen and educated women……..”
The Japanese opened three different ‘hospitals’ in the Moji area for POWs who had been so debilitated after their POW transport ships arrived they could not be sent to their intended POW Camp for work.
They were the Kokura Military Hospital in Kokura, the Quarantine Station on Hakoshima Island in Shimonoseki, and the POW camp, Fukuoka 4B, in Moji.
Each facilities coame to be known as ‘Moji Hospital’ – leading to considerable confusion about where many Allied POWs were sent upon arrival in Japan.
Nearly all 350 POWs (British, American, Australian and Dutch) who died, did so within days or weeks of their arrivals in Japan. They were as much victims of the ‘Hellships’ as those who died during the journey.
Japanese medicine was at a primitive stage during WWII.The training and skills of medical Japanese personnel were many decades behind the standards of Europe or the United States. Most medicines that were available came from Allied Red Cross packages intended for POWs, however the Japanese kept most for themselves, leaving only small amounts to treat POWs.
These ‘hospital’ facilities were little more than aid stations where ill POWs could be isolated. Typical of the Japanese, Allied doctors and corpsmen were brought in when the numbers of sick and dying POWs became too great. American, British, Australian, and Dutch doctors and medics delivered most of the real medical care at these facilities.
KOKURA MILITARY HOSPITAL
This was the only real hospital and most commonly referred to as MOJI HOSPITAL. It was here following disastrous voyages that POW survivors were taken to.
More than 160 American, Dutch, and British POWs perished at Kokura Military Hospital due to the appalling physical condition of POWs and the minimal Japanese treatment offered.
Shimonoseki Quarantine Station
Located on Hakoshima Island, in the Enoura district of Shimonoseki, Honshu the station was built in1894 at the end of the Sino-Japanese war to isolate returning soldiers to prevent them from carrying infectious diseases to Japan.
In Nov 1942 the Japanese found themselves overwhelmed with the nearly simultaneous arrivals of Nagato Maru, Tofuku Maru, Dainichi Maru, and Singapore Maru – each carrying several hundred terribly ill POWs.
‘British officers performed triage on more than 100 POWs who lay awash in the filthy holds and bilges of Singapore Maru, sending those who they viewed as having the best chance of survival to the medical facility at Fukuoka Camp 4B in Moji. Eighty others were left aboard the ship awaiting the arrival of a medical party sent from Zentsuji POW camp.
The medical team, under Lt. Cmdr. T.I. Moe (USN Hospital, Guam), and including Lt. Cmdr. S.E.L. Stening (HMAS Perth), accompanied the patients aboard a junk across the Shimonseki straight to the Quarantine Station. Tragically, the men were in such terrible condition that 35 died before the survivors were transferred to the Yawata and Omine Machi POW camps in Feb. 1943.’
This is believed to be only time the Quarantine Station was used.
Fukuoka 4B POW Camp
‘Nov. 1942, the Moji YMCA building was converted into a temporary aid station to house more than 250 of the sickest British POWs from Dainichi Maru and Singapore Maru. Despite the arrival of medical assistance from Zentsuji POW camp, 120 men perished in the first two months. The Japanese made the YMCA building and its surrounding yard a permanent POW work camp. The survivors of the original group were joined by Dutch, American, and additional British POWs and laboured for shipping, railroad, and other companies in the Moji area.’
We wish to acknowlege Peter Winstanley’s website and thank him for the information https://www.pows-of-japan.net/
This included many years of research by Peter and statistics and conclusions are his.
The late Peter Winstanley acknowledged the POW Research Network Japan, records and rosters of Dutch POWs available at Henk Beekuis’s website. Electronic copies of Dutch POW record cards from the Netherlands National Archives which provided important confirmatory information. They can be accessed by following the “Japanse interneringskaarten” link on the Dutch Archives website. A short online biography of Australian doctor Samuel E.L. Stening, who worked at Shimonoseki Quarantine Station was also very informative.
Also the late Roger Mansell graciously provided numerous useful documents. Particularly important were files on Fukuoka 4B and the Dainichi and Singapore Marus from Record Group 331 Box 921. Rosters of Singapore Maru victims and survivors from the British Imperial War Museum (WO 208/4282), via Mr. Keith Andrews, were also generously provided by Mr. Mansell. The rosters can be viewed at Mr. Ron Taylor’s Singapore Maru Roll of Honor, as well as at Roger’s “Moji Military Hospital Camp” page. Please note that the current (Sept 2011) version of Roger Mansell’s website illustrates the continuing confusion about the identify of “Moji Hospital.” The Rosters, affidavits, photographs, and links represent an intermingled mishmash of materials covering Fukuoka 4B, Kokura Military Hospital, and Shimonoseki Quarantine Station. I hope that the present website will help clarify what happened to the POWs who had the misfortune to be assigned to one of those facilities.
Sydney born Ewan Corlette was working at Orange when he enlisted as a Captain AAMC (as a specialist he was then promoted to the rank of Major) and was allocated to the 2/2 Casualty Clearing Station (CCS) serving first in the Middle East. On 18 February 1942 an element of 2/2 CCS, along with 2/3 Machine Gun Battalion and 2/2 Pioneer Battalion, moved to the Netherlands East Indies and landing in Batavia, Java. This was to honour a British undertaking to assist the Dutch to resist the Japanese. The Dutch stopped fighting on 8 March and with all the Allied forces, Corlette became a POW of Japan on12 March 1942.
The 2/2 CCS on arrival on Java, was under the command of Lt Col Norm Eadie who was then appointed Assistant Director Medical Services (ADMS) for the Java force known as “BlackForce”. As a consequence Major EE (Weary) Dunlop was made CO of the CCS and promoted to Lt Col (Temp). These CCS personnel became POWs and it seems that apart from Lt Col Eadie only 3 of their Medical Officers were in Java. They were:
Lt Col Dunlop and Majors Moon and Corlette. Major Jock Clarke, a dentist from 2/2 CCS, was also present and a 4th Australian Medical Officer, Captain McNamara from the 5th AGH, was attached.
Subsequently, a hospital facility was established and it is assumed that the CCS ceased to operate. The former CCS officers, plus RAF and RAMC personnel, who had also been captured, staffed the hospital.
We wish to acknowledge the above information is copied from the late Peter Winstanley’s website: https://www.pows-of-japan.net/articles/28.htm
At the Australian POW Memorial in Ballarat in 2018 and the 14th Anniversary Service the Guest Speaker was Andrew Corlette, son of Ewen Corlette, one of the Australian doctors captured in Java and sent to Burma-Thai Railway. The following is the address by Andrew Corlette
At sea 13 Oct 1945. Medical officers of the Java Force, released prisoners of war (POWs) of the Japanese, aboard the British troopship MV Highland Brigade during their journey home to Australia.
Left to right: WX11120 Lieutenant Frederick George Smedley, 1 Java Ambulance Car Unit, Australian Medical Forces (AMF); WX11057 Captain Theodore Godlee, 2/3rd Machine Gun Battalion; VX14845 Lieutenant Colonel Norman Menzies Eadie, Assistant Director of Medical Services, Java Force, AMF; Lieutenant Colonel A C King, 1 Mobile Field Ambulance; NX350 Major Ewan Lawrie Corlette, 1 Allied General Hospital; Major J E R Clarke, 1 Allied General Hospital; TX2185 Captain Tulloch Graham Heuze Hogg, 13th General Hospital; Major D F Murphy, 2/10th Field Ambulance
At sea, 13 Oct 1945. Medical officers of the Java Force, released prisoners of war (POWs) of the Japanese, aboard the British troopship MV Highland Brigade during their journey home to Australia.
Left to right: WX11120 Lieutenant Frederick George Smedley, 1 Java Ambulance Car Unit, Australian Medical Forces (AMF); VX14845 Lieutenant Colonel Norman Menzies Eadie, Assistant Director of Medical Services, Java Force, AMF; Lieutenant Colonel A C King, 1 Mobile Field Ambulance; NX350 Major Ewan Lawrie Corlette, 1 Allied General Hospital; Major J E R Clarke, 1 Allied General Hospital; Captain Theodore Godlee, 2/3rd Machine Gun Battalion.
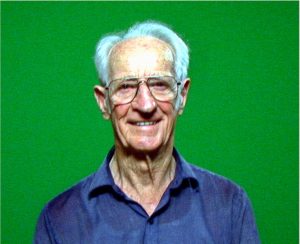
John Chalmers was born in Sydney on 20 March 1910. He went to high school at Fort Street Boys High School and studied medicine at Sydney University. He also served in the Militia as a member of Sydney University Regiment for a number of years.
Following graduation in 1936. Dr John S Chalmers was a resident doctor at Royal Prince Alfred Hospital in Sydney. He married Mary Violet O’Keeffe in Sydney during 1937. He and his wife moved to Hobart where he became the Registrar at Royal Hobart Hospital (see later comment where it is suggested that he was Assistant Superintendent).
The 2/4 Casualty Clearing Station (CCS) was raised in Hobart late 1940. John enlisted in the AIF on 26 August 1940 as a Captain Medical Officer. Lt Col Thomas Hamilton was appointed Commanding Officer (CO) of the CCS on 15 November 1940. Whilst moving from Newcastle to take up his appointment at the CCS in Hobart, he had attended a Conference in Melbourne and had the opportunity of visiting a training establishment at Royal Park Depot. There he saw Major J.S. Chalmers in action. He was impressed. Following intense lobbying by Lt Col Hamilton John was appointed to the CCS.
“8 December. I worked till midnight last night then suddenly felt tired. John Chalmers, the fair haired young doctor whom you met in Hobart, located me on the veranda. Presenting me with a half mug of rum and a cheerful face he said: “Major Krantz and I have prescribed a snifter. It might help you along sir!”
John Chalmers, later fated to die heroically by enemy action, had a passion for doing good by stealth. Australia has produced many fine soldier-doctors but, among the younger group, I knew of none finer than Chalmers. Assistant Superintendent of the Royal Hobart Hospital in civil life, backed by seven years experience as a militia officer, he was one of those useful all rounders who gladden the heart of a hospital commander. His knowledge of x-ray work was especially valuable.
Major Chalmers, always an early riser, was up and about. I saw him, dressed in pyjamas and steel helmet, conferring with Private Lockwood, the air defence picquet, at the other side of the garden.
Major Fisher will be in charge of the resuscitation and transfusion teams. Captain Brereton will assist him. The Padres will work with Captain Higgin in the reception tents and Major Chalmers will assist with the anaesthetics until required in the X-ray department.
In the reception tents, which were filling rapidly, Captain Higgin and Major John Chalmers moved busily up and down the rows of stretchers supervising the classification of the patients, most of whom bore Field Medical labels with a brief description of their wounds. Two or three benches near the entrance were filled by “sitting” or “walking” cases. Eagerly they accepted the mugs of steaming cocoa, the biscuits and the cigarettes offered them by the two padres who evidently were determined to make a hard working night of it.
Sniffing the cocoa, a boyish young officer on a nearby stretcher raised himself on one elbow. “Gosh!” he ejaculated, “I haven’t had a feed in three days.” Through the grime of his unshaven face I recognized a well-known infantry subaltern. “Well we may be able to remedy that,” I said as I checked the Field Medical card pinned to his shirt. “Flesh wound through left thigh, no haemorrhage. That shouldn’t prevent you eating at any rate.” Sending round to the cook house I procured for him a plate of hot M and V, the famous army meat and vegetable ration which can be very appetising to a hungry man…….Recognizing the lieutenant also, John Chalmers found time to bring him a tot of whisky. “This’ll put hair on your chest,” he said. Sniffing the glass, a gleam entered the lieutenant’s eyes followed by a spreading smile on his pale face as he downed the contents. “This is Heaven! I always did like the Army Medical Corps, “he remarked.
In the adjoining room Captain Michael Woodruff was busily unpacking jars of blood serum. In Major Fisher’s absence Michael had taken charge of the resuscitation of shocked patients before and after operation, a life-saving job. I nodded towards the jars: “Likely to need any of them tonight, Mick ?” Pausing in his work, Michael straightened up. “I hope not, sir. Major Hobbs tells me from the theatre that all goes well.” Content with this news I went down the covered way to the theatre where Alan Hobbs and his team of orderlies were hard at work. The indefatigable John Chalmers was now administering anaesthetics. The heat was terrific, for the brilliant light was screened from outside by a couple of army blankets hung over the doorway.”
“Leaving Bukit Panjang after lunch I found John Chalmers working vigorously at our new site. Stripped to the waist in the hot afternoon sunshine, his head shaded by a battered felt hat, he not only directed the incoming trucks but helped to manhandle the equipment. Momentarily free from the threat of artillery fire, the men worked with a will on the tents erecting so many by tea time.”
We were not at all happy. From the depths of a deck chair a cynical wag remarked: “Well boys! Black Friday tomorrow! It’s the thirteenth of February.” “Oh, shut-up!” said the misanthrope on my left. “If we had any sense we’d collar that little Chinese ship out there and clear off ourselves.” “You’d blow yourselves up on the land mines before you got through the barbed wire”, said John Chalmers, who had joined the group. “Anyway, what about the wounded blokes up in the building there? Who’s going to look after them?”
“Majors Fisher and Chalmers, with the rest of the Casualty Clearing Station, had the adjoining Convent filled with medical cases. In order to be near their patients, they moved down into a little bungalow at the Convent gate”………
On 15 February 1942 the Allied servicemen became Prisoners of War (POW). Then in May 1942 3,000 Australian POWs, including 12 Medical Officers plus medical orderlies, were sent to Burma on two approx 500 tons ships, otherwise described as Rust Buckets. They sailed from Singapore in two ships the Celebes Maru and the Toyohashi Maru. At Medan in Sumatra, the convoy was joined by another vessel, ironically the England Maru. On the England Maru were 500 British soldiers and unexpectedly one Australian – Lt Col (later Sir) Albert Coates. The convoy then moved to the coast of Burma and left 1,000 men at Victoria Point, Mergui and Tavoy. Medical teams, including 2 or 3 Medical Officers, were left at Victoria Point and Mergui with the balance going on to Tavoy. At Mergui the Australian (AIF) POWs were under the Command of Lt Col Ramsay.
Major John Chalmers and Captain Thomas Brereton were left at Mergui with the Australian POWs. The British POWs, including Lt Col Coates from Sumatra, were also left there. Major Chalmers wrote a critical report on the conditions experienced during the nine day journey. The main points were, amongst other things, the inadequate latrine facilities, limited drinking water, inadequate sterilisation for eating utensils, crowding in the holds (especially when at Medan an additional 350 Japanese troops boarded). The move from Mergui was made in August 1942 when the POWs were moved up the coast to Tavoy in vessels no larger than Sydney Harbour ferries. Ultimately construction of the Burma Thailand Railway commenced from a place called Thanbyuzat in Burma in October 1942.
The 12 Medical Officers of “A” Force, plus Lt Col Coates, were deployed amongst the working parties (mobile teams) on the Burma end. Major Chalmers was at Thanbyuzat Base Hospital Camp, Apparon Camp (about 82 km from Thanbyuzat) and Kun Knit Way-55 kilo Hospital Camp. There are probably other locations of which we have no knowledge.
When the railway was completed in October 1943 the Burma work parties which comprised the original “A” Force, and other groups which arrived later, were moved down to Thailand. About late 1943/early 1944. The actual camps that John Chalmers was at in Thailand is not clear.
What is clear is that he became part of the “Japan Party” and, as such, he was en route to Japan in Saigon in June 1944. The following an extract from the British Battalion Diary for portion of June.
22nd Electric Light failed p.m. Musical instruments sent in by local French Red Cross. 23rd Brigadier Varley, Capts. Sumner, Stewart and Richards with 35 Kumi and part of 36 Kumi left for Singapore via Phnom-Penh. 24th Capts. Burk, Phillips, Chalmers with 37 Kumi and part of 36 Kumi left for Singapore. R.C. trouble. 25th Capts. Flinn and Campbell-Smith with 77 men from 38 Kumi, 40 men from 40 Kumi, and all 39 Kumi left for Singapore. Rain fell all day. 26th Capts. Moore, Higgins, Fleming with remainder of 40 Kumi and all 41 Kumi left en route Singapore. An Australian from 50 Kumi left with the party. Trouble with Jap office staff.
The names typed in bold are Medical Officers and Capt Fleming is a Chaplain.
The move to Japan through Saigon was abandoned as the waters in that area were too dangerous. In June the Japan party was then sent south to Singapore. After some time on Singapore the Japan party boarded ships bound for Japan. The Rakuyo Maru was one of these. On 6 September 1944 the convoy put to sea. On the night of 11/12 September the convoy came under attack by American Submarines. The Rakuyo Maru was torpedoed. We have some first hand accounts of John Chalmers last hours alive.
“…. Soon there were fifteen men clinging to this raft, including the Tasmanian doctor Major Chalmers”
“ The doctor-Major Chalmers came by wearing a life preserver. He was ill. Malaria. It had cycled on him while he was in the water. He was shivering and shaking. We invited him to get on our raft. He got on, but two or three hours later, he died. We pushed his body off into the sea.”
There is a further account about a Medical Officer’s death following the sinking of the Rakuyo Maru in the book “Bamboo and Bushido” by Albert Albury published 1955. In discussion with a survivor of that sinking Dr Rowley Richards (who has published his book “A Doctors War” ISBN 0 7322 85321 published 2005) it is agreed that this is almost certain to have been an account of the last hours of John Chalmers life.
“Late in the afternoon of the fourth day Ted and I came across the doctor drifting alone on a hatchboard. He was delirious. He had dysentery, and I could see that he was dying. We pulled him on the raft and sat either side of him so that he could not roll off. He kept asking for water. His bottle, of course, was empty . I dipped my hand into the sea and let a few drops splash into his mouth. It would make little difference to him now if he drunk it or not. Once or twice we had to hold him down as he found a little strength in his ravings. But as darkness came he lay quiet, unmoving. In the torpor that came with the night we forgot he was there.
Throughout the early hours of the next morning I kept on falling across him, forgetting who or what his body was. It was something to rest my head on. At dawn we found he was dead. And as I looked at him, his mouth agape, his face a thousand years old, his eyes still fixed with pain and delirium, I remembered all he had done for me, and for so many others. And for a few moments I became a human being, and was filled with sorrow and compassion. He was one of the finest men I had ever known.………We rolled his body off the edge of the raft.”
CO Lt Col Hamilton in his book wrote these comments about John Chalmers.
“As usual, John (Major Chalmers) had been the first to volunteer as medical officer for the draft . They sailed from Singapore for Japan in an aged, filthy hellship, the Rakuyo Maru, which bore no international markings to indicate she was crowded with defenceless prisoners. On 12th September 1944, an American torpedo pierced her guts and the depths of the China Sea claimed hundreds of weakened men. Struggling swimmers were crushed under the propellers of racing Japanese destroyers, but some were lucky to survive until picked up by the submarine four days later. Arthur Varley was last seen in the water the second day. John Chalmers died after two days of thirst and exposure on a raft. Private Brettell, a fine little English orderly from my unit, and Lance-Corporal Barrow also died.
Vale John Chalmers! Always his brother’s keeper, he was a man to inspire and guide the helpless.
Or would he have laughed outright if anyone had told him so? Almost, one can picture him under a burning sun on that frail raft, whispering through cracked lips before he turned in his final report,”
“Here, take my possie mate. It’ll make things a bit easier for you.”
Informal portrait of members of the 2/4 Casualty Clearing Station. Identified, left side of the table, front to back, NX70505 Lieutenant-Colonel (Lt-Col) Thomas Hamilton, Captain (Capt) Furocer (?), Lt Robinson and SX10761 Major (Maj) Alan Frank Hobbs. Centre back is 240062 (NX70685) Padre Frederick Hugh Bashford. Right side of table, front to back, TX2150 Capt John Sneddon Chalmers, Maj Phillips, TX6009 Capt Edgar Newton Lee and NX70473 Padre Bernard James Quirk. ****Capt Chalmers, (later major), died at sea, while a prisoner of war, on 14 September 1944.
The above information was compiled by Peter Winstanley for his website we wish to acknowledge his generosity using his research and writing.
The following extract is from papers given to Lt. Col. Winstanley by the daughters of Lt. Col. Thomas Hamilton – Jean Charlton (Newcastle) and Anne Mulholland (Melbourne).
LT COL THOMAS HAMILTON COMMANDING OFFICER OF 2/4 CASUALTY CLEARING STATION AT THE FALL OF SINGAPORE.
Author of his book ‘Soldier Surgeon in Malaya’ published in 1957 by Angus & Robertson – Page178-180 has the below story.
Following capitulation he recorded the verbatim accounts of some of the men he treated in Roberts Barracks Hospital. By coincidence he also made the following verbatim record of the experiences of a Japanese officer who was involved in crossing the Johore Straits and coming under heavy machine gun fire from the Allies. This fire would almost certainly have been from some of the 2/4th machine guns on the coast west of the Causeway. Colonel Hamilton was Senior Medical Officer with ‘A’ Force Burma – the first body of Australian POWs to leave Singapore to work on the Burma end of the Burma-Thai Railway 1942.
“This section was vividly related to Captain Lee (Adjutant of 2/4 CCS) and myself in the rat-infested hold of the hell ship ‘Celebes Maru’ during a hot night in late May 1942 when the ship – deserted except for a portion of my unit and a few Japanese guards – lay at anchor in the Gulf of Tavoy. Sasaki, unusually decent and generous to us, spoke fairly good English. He wanted to talk of Western classical music, but we drew him on to speak of Singapore, the while munching on a tine of bully-beef which he had brought to us.
Lt (Choi) Sasaki aged 23 years, a fighting wild-cat of a machine gun officer in the Imperial Nipponese Army demonstrated with flashing eyes and vehement gestures how his military landing craft had started from the south western corner of Johore and proceeded at full speed with lights showing, towards the Causeway. When fire was drawn from the defenders on the opposite side of the narrow strait, the lights were extinguished. Then the motor barges were turned about and steered back to a pre-selected landing place on Singapore Island.
“It was ver’ bad place” continued little Sasaki, his voice rising as he recalled the excitement. “Orstralians shoot ver’ hard, ver’ fast, brr’p, brr’p (imitating the rattle of machine guns) “so that Nippon soldiers jump down” among mangroves “and sweeem, sweem in mud, oil and dark. Hoi! Hoi! What a beeg mess! We throw off packs, off shirts, off everything except sword and material for fight. Then we fight with glory in mud. Ah! Orstralians! They are for me a grand souvenair of fight for Seengapoor – what you say? A gallant memory.”
“When morning come we have crawled to railway line past mangroves. When I look up – all quiet! About feefty metres away I see road where like many dead men er.. er.. p’raps twenty-seeven Orstalians, ver’ sad, ver’ sad! Here Lieutenant Sasaki stood erect at the salute). “I give them salute of honour. Then on to objective, more fight begin, grand fighting but no water, no food! For five days we drink from stream and eat cocoanut; dam’ near starve! But on feefth daty take Mandai Hill where we rest ah! Beautiful rest. Never forget Orstralians and grand fight souvenair they give me at Seengapore.”
Marvelling at the stamina revealed by Sasaki’s men between the landing and the capture of Mandai Hill I could not help asking: “And where did you train for all this fight, Choi?”
“Ah! French Indo Cheena,” he answered readily. “Every day for six months, twelve hours every day, dig jungle, sweem swamps but keep sword and guns clean, ver’ hard!”
Sasaki had too much regard for our feelings to add that the Japanese were good fighters. No white troops would stand such a hard, animal-like training; but jungle warfare and animal life have much in common.
The casualties caused by the Japanese landing meant more work for the Medical Service; while the civilian and military inhabitants were startled into a frenzied activity paralleled only by that of an ant heap into which a stick has been thrust.”
New reinforcements still arriving from Australia and India were wasted for there was time to train the men in the type of warfare the situation demanded. Sixteen hundred Indians-rustic types arrived in the charge of six Indian jemadars (junior officers or a former rank in the Indian Army the lowest rank for a viceroy’s commissioned officer.) all wearing heavy winter clothing. They were handed over to experienced engineers for road-construction work. Frank Wayman a senior engineer said that about 800 could be mustered for work. Most of them were adept in evasion when confronted with a pick and shovel.
Many of the Australian late-comers were no better. Col Anderson VC who received 620 reinforcements to fill the defeated ranks of his hard-pressed batallion told me that scores of them did not know how to load a rifle, while hand-grenades and mortars were absolute mysteries.
Informal portrait of members of the 2/4 Casualty Clearing Station. Identified, left side of the table, front to back, NX70505 Lieutenant-Colonel (Lt-Col) Thomas Hamilton, Captain (Capt) Furocer (?), Lt Robinson and SX10761 Major (Maj) Alan Frank Hobbs. Centre back is 240062 (NX70685) Padre Frederick Hugh Bashford. Right side of table, front to back, TX2150 Capt John Sneddon Chalmers, Maj Phillips, TX6009 Capt Edgar Newton Lee and NX70473 Padre Bernard James Quirk. Capt Chalmers, (later major), died at sea, while a prisoner of war, on 14 September 1944.
A group portrait of allied and Japanese medical staff outside a disused police barracks at Tavoy, Burma, where 2/4th Casualty Clearing Station ran a small hospital. They shared their quarters with three Dutch doctors from Sumatra. ‘A’ Force was building an aerodrome nearby. Front row (L to R): Four Japanese doctors; a Dutch doctor; NX 70505 Lieutenant Colonel Thomas Hamilton. Back row (L to R): TX6009 (T253515) Captain Edgar Newton Lee from Hobart; SX10761 Major Alan Frank Hobbs from Adelaide; Donald Murchison (Red Cross Officer); two Dutch doctors.
2/4th Australian Casualty Clearing Station was formed in Hobart, Tasmania in December 1940 and then moved to Brighton for training.
In January 1941 they moved to Melbourne to board a ship for Malaya and on arrival there established facilities at Kajang. In September they moved to Jahre Bahru where they established a small hospital before being relieved in November and then moving to the civil hospital at Kluang.
When the Japanese attack began in December they moved back to Kulai in January 1942 before retreating to Singapore where they were first set up at Bukit Panjang. After the Japanese landing on the island they moved to the Swiss Club and then to St Patrick’s College where they worked with the 2/13th Australian General Hospital until the surrender when they moved to Changi.
While the male members continued to work during captivity it was not as an organised unit.
Sixty five Australian nurses and over 250 civilian men, women and children evacuated on the Vyner Brooke from Singapore, three days before the fall of Malaya. The Vyner Brooke was bombed by Japanese aircraft and sunk in Banka Strait on 14 February 1942. Of the sixty five nurses on board, twelve were lost at sea, twenty two survived the sinking and were washed ashore on Radji Beach, Banka Island where they surrendered to the Japanese, along with twenty five British soldiers. On 16 February 1942 the group was massacred, the soldiers were bayoneted and the nurses were ordered to march into the sea where they were shot. Only Sister Vivian Bullwinkel and a British soldier survived the massacre. The remaining thirty two nurses who also survived the sinking were captured as POWs, eight of which later died in captivity.
One hundred and fifteen members of his unit were captured with 5 of the nursing staff being executed on Banka Island, and three men drowning when the SS Rakuyo Maru was sunk by an American submarine as they were being transported to Japan. Eight died in Burma of illness or by accident.
In World War II, a Casualty Clearing Station (CCS) was a military medical facility located behind the front lines, tasked with treating and stabilizing wounded soldiers before they were transferred to field or base hospitals. They acted as a crucial link in the evacuation chain, providing initial care and preparing casualties for further treatment or evacuation.
CAPTAIN BOOTH’S REPORT
(This report by Captain E.H, Booth 2/30th Battalion AIF was handed to Major Charles Green 2/4th MGB. Item donated by daughter of Charles Green, Mrs Brand.)
The 2/30th Infantry Battalion formed 22 November 1940 at Tamworth, New South Wales, with men drawn from Dubbo, Goulburn, North Sydney, Randwick, Wallgrove, and Wagga Wagga. The first 2/30th commander, Lieutenant Colonel F.G. “Black Jack” Galleghan, trained the men hard and they became known as “Galleghan’s greyhounds”.
The battalion was part of the 8th Division’s 27th Brigade, the last AIF infantry brigade raised for service during the Second World War.
The following is a copy of a communication received from Capt. E.H. Booth, Commander of ‘D’ Company 2/30th Battalion addressed to Major Charles Green 2/4th Machine Gun Battalion:
Following are the details of the engagement of my Company with the enemy on 12th February 1942 in which Lieutenant G. MacKinnon who was attached with his Platoon and four guns displayed outstanding courage and devotion to duty and in my opinion deserve some sort of recognition for this.
On the morning 11th February 1942 the 2/30th Battalion withdrew under orders from the Causeway sector to the vicinity of Mandai’s crossroads and occupied a new defensive position with companies disposed from crossroads to the Singapore-Malaya pipeline astride the road. ‘D’ Company position was such that it was responsible for protection of the right flank of 2/30th Battalion and as the most likely method of enemy approach appeared to be along the pipeline the Company was disposed along this and on the forward slopes of the high ground just north of Mandai Road at this point.
Lt. MacKinnon’s platoon with 4 medium machine guns at this stage came under the command of ‘D’ Coy 2/30th and the co-operation, intelligence and energy of MacKinnon and his men was noticeable from the start. MacKinnon himself made many reconnaissance missions in order to find the best possible gun positions for the tasks I gave him and throughout the whole day of the 11th February he spent his time improving the general fire plan of my position. After reconnaissance patrols at night and a fighting patrol at dawn made contact with the enemy north and along the pipeline at 0910 hours 12th February he launched a heavy attack in the general direction south along Sungei Mandai and on ‘D’ Company’s position.
This at this time 2/30th Battalion were in the process of carrying out an orderly withdrawal (not in close contact) with the object of counter attacking Bukit Panjang further south. ‘D’ Company automatically became a vanguard for the Battalion and much depended on the time we could hold off the enemy attack. MacKinnon had to bring his guns back from the trucks at great speed and under fire. These guns were remounted and maintained in action despite heavy fire and some casualties for nearly two hours for which period the position was held. MacKinnon himself proved fearless under fire, personally directing the fire of the guns on many occasions.
When an Indian Regiment on our right flank was known to have withdrawn east along Mandai Road I decided to withdraw and it was not until every man of my company was successfully out of the position that MacKinnon brought his guns out. He did everything possible to save these guns but by the time they were loaded on his truck and his Platoon Sergeant (Sgt WX8809 Richard Sandilands) had been killed during the process he was about completely surrounded by the enemy and I consider he did the only thing possible when he had to finally abandon them after attempting to destroy both truck and guns in the face of enemy fire.
The final withdrawal of his men across Bukit Mandai whilst under exceptionally heavy fire was also a tribute to the courage and outstanding leadership of Lt. MacKinnon.
The 2/4th 8 Platoon MGB soldiers who died in and around Mandai Hill on that day:
The following has been copied from the Nigel Mansell website. We wish to acknowledge and thank them.
Niihama had 245 Australian POWs of which three died. Ranking man was Lt. Peter Selwyn Withycombe (NX70315) from 2/15th Field Regiment, 8th Division raised in NSW. Photograph below:
Cholera isan illness that gives you severe diarrhoea and dehydration. It’s found in areas of the world with poor water and sanitation. Cholera usually followed the monsoonal rains.
A seriously poor diet contributed towards tropical illnesses such as cholera
Treatment – Rehydration. The goal is to replace lost fluids and electrolytes using a simple rehydration solution, oral rehydration salts (ORS).
‘It was shocking the way cholera could hit in such a short time. When cholera showed up the person passed grey slime from both ends, it just seemed to take all the fluid out of the body. When anyone died of cholera if they fouled their gear, blanket or anything else they whole lot went out, everything was burnt. They would build up a great big fire on a base of logs to get a fire burning that went for days at a time. And the bodies of the cholera deaths were burnt – there was not much left when they passed on. Those that were too sick to go out and work got the job of burning the bodies. They would have two poles, drop a body across the poles and then run in towards the fire and throw the body in, then get back as quick as you could because of the heat of the fire. It was strange, you would throw a body on the fire and all of a sudden you would see his arm come up or a head shift or some other movement. The heat of the fire pulled sinews in the body and caused the movement but it was a terrible, terrible thing.’
From WX17634 Wally Holding, 2/4th.
Cholera was the most feared tropical illness of all POWs and Japanese in Burma/Thailand. A POW could die within hours.
The doctors began strict regimes to boil all drinking water. Eating and cooking utensil and plates had to be dipped into boiling water before use.
The following is from an interview with Dr. Phil Millard in 1991
‘Apart from the diarrhoea and vomiting the dehydration is a peculiar thing. It manifests itself by wrinkling of the finger tips, like a person who’s had their hand in water for a long time and it is quite typical and I’ve never seen it in a dehydrated patient anywhere else. But it’s very distinctive. The other thing is huskiness of the voice and I suppose it is, again, dehydration of the larynx. So these two things I even have seen a patient who feels he’s taken ill, he gets the husky voice and the wrinkled fingers actually before the diarrhoea comes on. Now that in at least one case I can remember that happened.’
13 Soldiers from 2/4th died of cholera on the Burma-Thai Railway in 1943. Several other POWs contracted cholera however miraculously survived.
WX7569 Corp Stuart Edward FOXALL, was originally with 11 Platoon ‘C’ Coy. Captured Java about 8 March 1943. Sent to work on Burma-Thai Railway with Java Party No. 4, Williams Force.
Tragically Foxall contracted Cholera, died July 1943 at Beke Taung 40 Kilo Camp, Burma at the age of 22 years.
WX10366 Pte Norman Wilson FRASER driver with ‘C’ Coy left Singapore by sea to work on Burma-Thai Railway with ‘A’ Force Burma, Green Force No. 3 Battalion.
Died of Cholera at Aungganaung 105km Camp, Burma aged 29 years, , his illness began at 0830 hours on 4.6.1943 after drinking contaminated water. Norm was father of two children.
WX8674 Pte John Edgar James GREGORY Kalgoorlie boy and miner, worked Burma-Thai Railway with ‘F’ Force died cholera 1 June 1943 aged 39 years Shimo Sonkurai Camp, Thailand.
He enlisted just few weeks prior to his brother WX9202 Ronald Keith Gregory (also with ‘F’ Force, survived and recovered Singapore).
John & Ron Gregory Gregory
WX8250 PTE Francis (Frank) HALBERT b. Menzies, a prospector from the Goldfields. With ‘F’ Force on railway died cholera at Shimo Sonkurai 4 June 1943 aged 35 years at Shimo Sonkurai, Thailand, just a few days after Gregory died.
WX7628 Sgt Edgar (Tim)) Joseph HOWARD died 1 July 1943, aged 31 years of cholera Burma-Thai Railway with ‘H’ Force Malayan Hamlet, Thailand.
WX16392 Pte Gerry Brown KLUTH (OR CLUTH) labourer & professional cyclist, joined ‘D’ Coy 14 Platoon.
Whilst working at Kanu II Camp Gerry contracted Cholera and died on 5th July 1943 at the age of 23 years. Whilst in the cholera camp Gerry was next to another 2/4th soldier, WX8623Jim Gilmour. Jim miraculously survived his Cholera attack and years later returned home to his family.
Below: Jim Gilmour survived Cholera.
WX8425 Pte Edward (Ted) Johnathon LEADBITTER was with ‘D’ Coy 15 Platoon when captured by Japanese on West Coast but escaped to rejoin unit before surrender.
A former Fairbridge Farm Schoolboy, Ted had married just before departing WA. He left Singapore with ‘D’ Force V Battalion – a work force kept separate from other ‘D’ Force parties. They suffered terribly with illness and often desperate work and living conditions.
At Kuii Camp, Thailand Ted was suffering from malaria and was delirious. He was kicked and beaten for 30 minutes by the spiteful and vengeful Japanese Engineer Corporal known as ‘Black Cat’. Ted died of cholera 14 days later aged 24 years.
WX7640 Forrest LEE-STEERE driver with ‘D’ Coy HQ. A farmer from Bridgetown, he left Singapore with ‘D’ Force V Battalion to work on Burma-Thai Railway.He died Kuii POW Camp of cholera on 3 Oct 1943 aged 36 years.
WX8639 Pte Joseph (Joe) John LYNCH sent with ‘D’ Force S Battalion to work on Burma-Thai Railway. He died of cholera and typhus at Konyu 1 River Camp on 1 Aug 1943 aged 34 years. He was the only son in his family.
WX8621 Keith Kitchener (KK) McDONALD – departed Singapore by train with ‘D’ Force S Battalion. KK was working on hammer & tap with ‘Cowboy’ Matthews, with KK on hammer when he misguided the hammer onto the had of Matthews and suddenly collapsed. Taken back to Camp he was evacuated to Tarsau and died of Cholera 25 Nov 1943 aged 25 years.
KK’s brother WX8620 Clarence ‘Clarrie’ John McDonald was also a soldier with 2/4th, also sent with ‘D’ Force S Battalion. He survived to return home.
WX9052 Pte Henry (Harry) Elvin McDONOUGH sent to work Burma-Thai Railway with ‘H’ Force Group No. 3.
Departed Singapore Railway Station 3 May 1943 to Thailand and sent to Konyu II, Malayan Hamlet.
Conditions at the camp and work on the line was appalling. Deaths were frequent. On 27 June 1943, Harry unfortunately contracted cholera and died age 28 years.
WX8912 Pte Kevin George MOIR Rangetaker with ‘C’ Coy 10 Platoon, ‘Kev’ left Singapore to work on Burma-Thai Railway with ‘D’ Force S Battalion. He died 7 Aug 1943 at Hintokk River Camp of cholera aged 24 years.
WX7426 Pte John Patrick MURPHY enlisted AIF 6 Aug 1940, later joined 2/4th MGB’s Headquarters No. 2 Platoon Anti-Aircraft under C.O. Lt Royce. Royce and a large number of 2/4th were KIA or wounded at Hill 200 on 12 Feb 1942 including Royce.
Sent to work Burma-Thai Railway with ‘D’ Force V Battalion. Jack died of cholera 30 Nov 1943 at Kuii Camp, Thailand aged 27 years.
The misery POWs faced: during torrential rain – marching through mud, feet deep, without boots, without clothing to camps 30, 40 or 100 kilometres away or to work sites – unless you are really ill and cannot walk, you may have beri beri, malaria, dysentery or all three! But they don’t count when the Japanese need numbers.
Guards would march into the hospital tent and drag away any number of POWs to fulfil the numbers demanded by the Japanese engineers for the daily work.
DYSENTERY
What is dysentery?
‘acute Diarrhoea, that is passing motions or should I truthfully say blood, 30 to 50 times a day.’
Dysentery is essentially diarrhoea so violent it causes bleeding and death.
67% of all deaths at Tamarkan in 1943 were from bacillary dysentery.
It was one of the leading causes of death in Australian soldiers captured by the Imperial Japanese Army WW2.
Malaria and dysentery were especially common, with most POWs experiencing several attacks each year. Many POWs would suffer both dysentery and malaria at the same time. Dysentery and diarrhoea caused more than a third of prisoner-of-war deaths. Only critically ill were able to rest.
The continuous passing of stools caused dehydration and drained them of vitamins essential to their survival.
As told to Tim Bowden ‘Prisoners of War – Australians Under Nippon’ – The ABC series………………..
‘Toilet hygiene was the single most effective way to prevent cholera. Our doctor, Captain Millard, pulled no punches.
‘If you don’t make it to the latrine, you will infect some of your mates and they will surely die as a result of your carelessness and stupidity. If you get caught short on your mission you are the same as a murderer!’
Following instructions, we dug a new, very deep trench and placed four strong timber planks across it. We then cleared a pathway through the jungle scrub so that the latrine could be quickly reached by those in urgent need.’
‘In the never-ending rain the trench quickly half-filled with water and so to add to our lot, the area rapidly became muddy and the wooden planks precariously slippery. It was always a race against time. There were times when a man slipped,over balanced and fell into its murky depths.’
Konyu, Thailand. c. July 1943.`Dysentery Block’ of makeshift hospital set up in tents at H Force prisoner of war (POW) camp at Konyu 2 (later known as Malayan Hamlet), on the Burma-Thailand railway. H Force was a composite group of approximately 3000 British and 600 Australians. Their headquarters was set up at Tampie (*147 kilometres) and they were spread over a stretch of railway between Tonihan (*139 kilometres) and Hintok (155 kilometres), with the Australians at Konyu 2 (K2) (*152 kilometres). *Distances measured as north of Nong Pladuk (also known as Non Pladuk). H Force did not belong to the Thailand POW Administration, but was on loan from the Malaya POW Administration based in Changi. This problem of remote control caused enormous problems for its POW work force, which lost almost 28 percent of its members, including 179 Australians. The photograph is number 10 in a series marketed by the Far East Picture Company and originating from material used in the Rabaul War Crimes Trials. Original caption reads `10 – Dysentery Block, Kanya’. (Donor H. Clarke). With acknowledgement and thanks to AWM.
Can you imagine yourself as a POW ill with dysentery?
What would the pain be like? How would you feel with faeces all over and about you, lying beside another sick POW? Would you care if you lived or died?
Thinking about dysentery today, i.e. right now, I believe we immediately feel embarrassment. That is until we close our eyes and really imagine how you would cope. Remembering many of those around you are ill too!
Journal of Australian Military and Veteran’s Health
Volume 32 Number 3 – July 2024
DYSENTERY is associated with overcrowding, poor hygiene and warm climates. It is highly contagious and can be spread by just a touch.
There was extreme overcrowding in POW camps, with men restricted to the small area of allocated space for sleeping. Conditions were far worse during transportation on trains and ships (Hell ships to Japan and 3-4 day sailing between Java, Sumatra and Burma) and 4-5 day train trips in overcrowded trucks to Burma-Thai Railway.
However the POWs suffering malnutrition and exhaustion after years of incarceration were hardly able to fight off disease.
The folllowing are just some of the challenges awaiting Work Parties at ‘new’ campsites, (for many POWs they would have worked all day at the last Camp, packed up and walked all night and arrived at the new location and be ordered to work:
work party would have to construct a camp
remove the bodies of Romushas who died of cholera
water needed boiling before drinking –
latrines required construction
roofs and walls of existing accommodation repaired
existing camp sites flooded with mud & often faeces during rains
set up new kitchens and hospital wards
Below: POWs had to stand for hours every morning and evening at parades to be counted and for work parties. Imagine being ill, say with dysentery, you probably would have preferred death rather than try to stand while Japanese guards counted the number of POWs over and over again. Which they did often.
Were there enough men for today’s work party?
How many men did the engineers demand?
Above: POW on ground has beri beri is unable to stand, others have bandaged leg ulcers, POW with blanket around shoulders probably has malaria, how many have other illnesses, there are No boots and few clothes – but it is ‘off you to work you go’
Beriberi: A thiamine (vitamin B1) deficiency, associated with polished rice consumption.
The Burma-Thai Railway Doctors were excessive at times about hygiene, drinking water and latrines in POW Camps – far more than the British or Dutch. But it saved many lives.
Dysentery is commonly spread by dirty water or food being contaminated with human waste. With diarrhoea comes the threat of dehydration. Loss of water and electrolytes including sodium, chloride, potassium and bicarbonate are lost through liquid stools, vomit, sweat, urine and breathing.
The large Camp Hospitals had dedicated Dysentery (tented) wards.
Amoebic dysentery could be treated with emetine (acquired by Camp doctors usually obtained through Black Market) as there were no official medical supplies for POW Camps. Amoebic dysentery was considered to be more of a chronic condition which lingers and is debilitating.
At Thamby POW Camp in Burma there were 4 deaths of 2/4th men – three died of dysentery and at least 4 deaths of 2/4th men at Khonkan Hospital Camp.
DYSENTERY AMONG PRISONERS OP WAR: SINGAPORE 1942-45.
A Thesis for the Degree of M.D.
by Kenneth C. Hutchin, M.B., Ch.B.
Glasgow University.
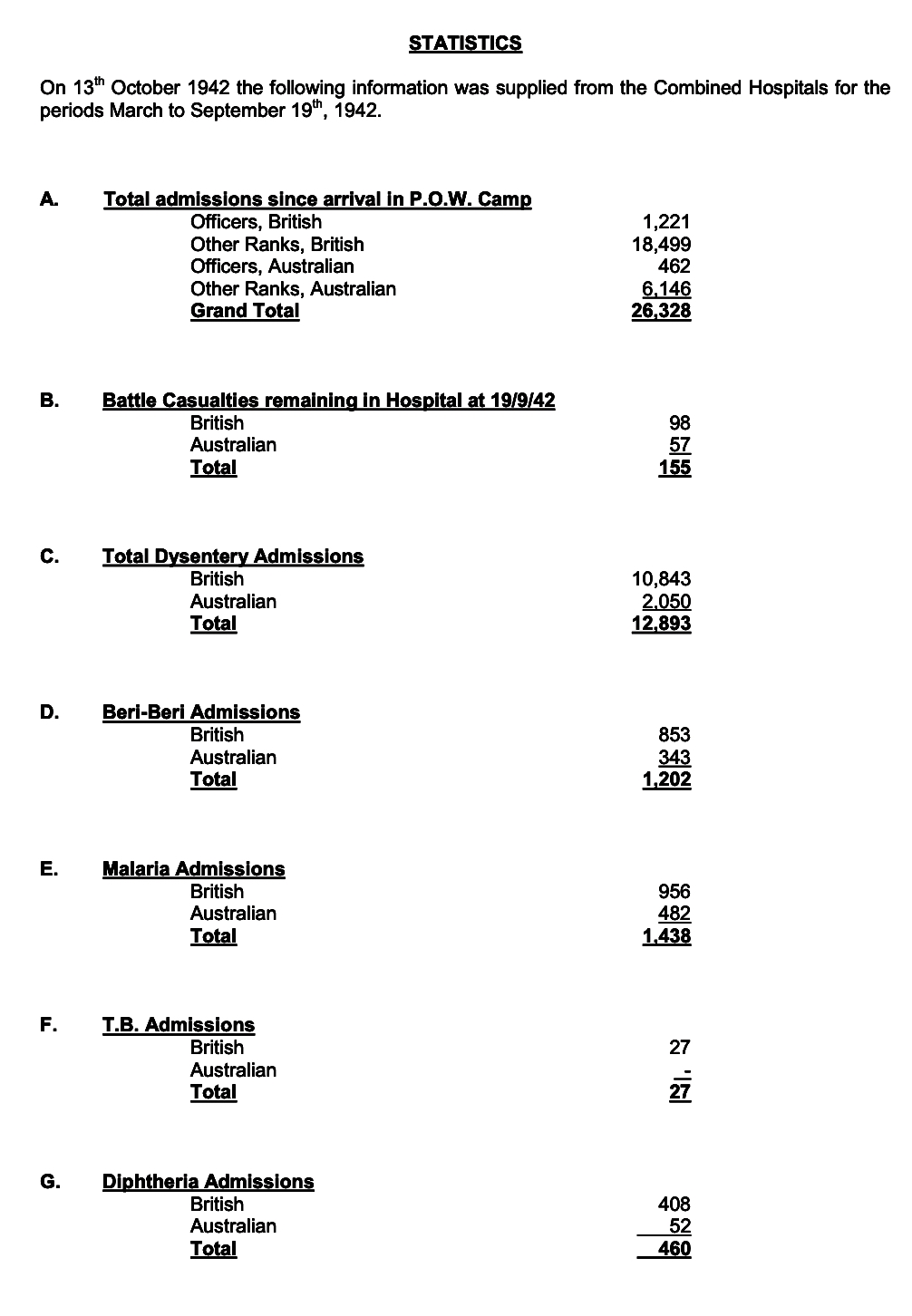
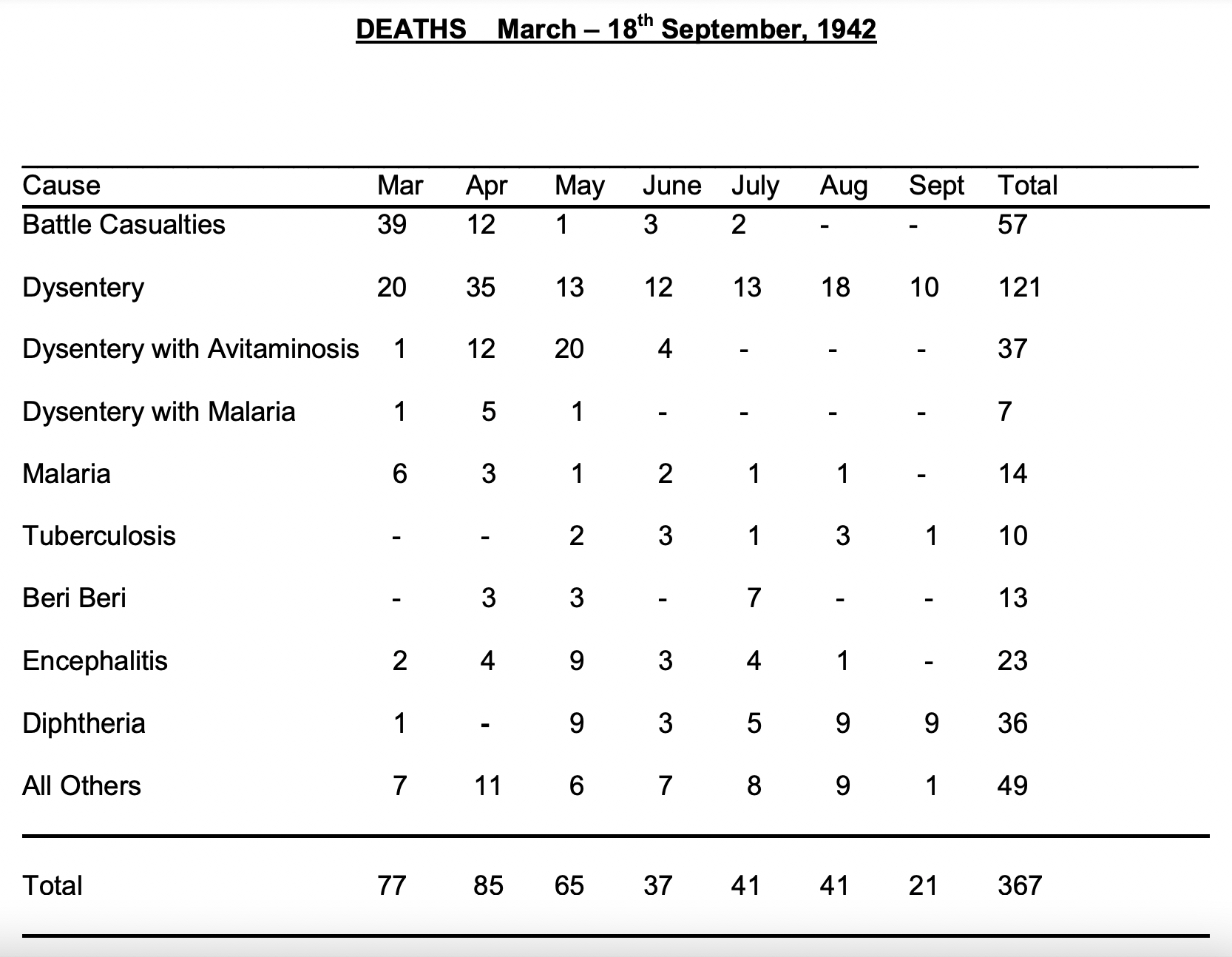
The largest epidemic of acute bacillary dysentery to occur in the Singapore P.O.W. Camps was the initial outbreak. The Dysentery Wing of the hospital was opened on 11th March, 1942. Two days later the total number of in-patients was 550* The number rose to 800 during the next two weeks and remained at that level for two months, after which the total gradually fell. Prom June to August the total was between four and five hundred. During the first five months 10,000 were admitted to the Wing: the deaths numbered about 120 and the chronic cases 100.
At the beginning of September the Selarang Episode caused a sharp rise in the number of cases of acute bacillary dysentery. The record total of 830 patients in the Dysentery Wing was then reached. This epidemic was not sustained to the same extent as the previous one and by mid November there were only 290 cases in the Wing including 30 amoebics and 90 chronic bacillaries. At the end of 1942 parties began to arrive from Java, and in these: many already dangerously ill with bacillary dysentery on arrival. This caused a fresh epidemic in Singapore during which the largest number of cases in hospital was between 400 and 500. The total number of cases admitted in 1942 was 15,000 and the deaths numbered 245.
During the first half of 1943 the average number of cases in the Dysentery Wing was 200 – When the hospital moved to Selarang in August 1943 there were only 140 cases of dysentery, including amoebics and chronic bacillary cases- At that time acute bacillary dysentery was only occurring as a sporadic disease – only one or two cases a week being admitted In December 1943 about 100 extremely severe dysentery cases of all types arrived from the Burma-Siam Railway working parties.
During the first half of 1944 the total gradually fell and only 40 amoebic cases and 40 chronic bacillary cases were in the hospital when it moved to Kranji at the end of May 1944 From then until September 1945 most of the acute bacillary cases were dealt with in Camp Hospitals at the various Working Camps.
At the Main Hospital in Kranji the number of acute bacillary cases in hospital at one time averaged about ten during that period. All these figures exclude Australian cases, as these cases, apart from those referred to the Sigmoidoscopy Clinic for an opinion, were always treated in a separate Australian Wing. The severity of the cases in the early epidemic of bacillary dysentery was extremely variable. All types from ambulant cases having a few loose stools daily to choleretic / cases in which death occurred in two to four days were seen. It was not possible to estimate the incubation period as the entire community was in more or less constant contact with infection from some source.
-00-
The above figures have been collated up until May 1942. The dysentery patients far outnumber all others. This graph has been taken from history of 13th AGH.
PATIENTS FROM JAVA
On October 11th, 1942, a group of prisoners, containing 362 Australians led by Major Robertson, 2/6 Field Company, sailed from Java to Singapore. On arrival many of these men were admitted to hospital.
Four Officers, 14 N.C.Os and 85 privates, mainly from 2/3rd Reserve motor transport, 2/2nd Pioneers, 2/6 Field Coy, Royal Australian Navy and 2/40th battalion were listed on the nominal roll of No. 3 and No. 4 Java parties presently
in hospital.
These men needed attention for malnutrition, dysentery, malaria and beri-beri. The whole Java Force left for Burma on 9th January, 1943 in much better shape than when they arrived at Changi.
What is the difference between amoebic dysentery and bacillary dysentery?
They have different causes.
There are two main types of dysentery: amoebiasis and bacillary dysentery (without medication the patient dies within two days).
Parasites cause amoebiasis, including E. histolytica, B. coli and strongyloidiasis. Bacteria cause bacillary dysentery, including Shigella, Salmonella, Campylobacter and E. coli.
2/4th Deaths:
22 Dysentery
8 Dysentery & Malaria
19 Dysentery & other illnesses.
Of interest, there were 53 deaths from Malaria and another 10 from Malaria in combination with other illness/s.
This includes numerous deaths at Sandakan and on the track to Ranau where Japanese guards would diligently write ‘Malaria’ as cause of death whether it was so or not.
The above figures are from history of 13th AGH.
An injection of Emetine as experienced by the great “Weary” Dunlop.
Extracts from “The War Diaries of Weary Dunlop”, Sir Edward Dunlop describes his experience of suffering from amoebic dysentery at Hintok in Thailand.
“25 May 1943 ….bang, down I go with dysentery, really quite severe. Trying to carry on and have not completely reduced my diet to fluids but have begun M. & B. 693 4g in about 10 hours. 28 May 1943 I am properly ill today with fever and nausea and severe abdominal pain, aching back andweakness. Dysentery intermittently which means slushing outside in the pouring rain and mud….I am eating nothing, fluids just a bit, M. & B. 693 continued 2-3 times a day. I have a hunch that I have really got amoebic dysentery and have had it for some time. 29 May 1943 Pouring rain and wet. I am feeling wretchedly ill….just able to take a little sugared drink. Continuing on M. & B. 693 one four-hourly with no effect. 30 May 1943. Still feeling very sick. Dysentery only slightly less. No lessening in blood and mucus….I am increasingly convinced my affliction amoebic dysentery… 31 May 1943 I am still a cot case, eating almost nothing… 1 June 1943 I took the plunge today and injected myself with emetine hydrochloric grains 1 *
* I collapsed under a tree going to the interminable benjo ( trip to the latrine)
The vultures gathered on the branches above, ignoring my feeble fist-shaking.
There arrived from nowhere Capt. “Legs” Lee RAMC, who felt my pulse and said he would give me some emetine.
I said: ‘Rot – how much emetine have you got?’.
He said ‘I have six grains and you will have half.’
I said ‘No way – you will need all that yourself.’
He gallantly over-rode me and prepared the injection, dissolving the tablets on a spoon.
The following day I was sufficiently improved to throw stones at the vultures!”
M & B 693 Tablets
Clear glass bottle, corked, containing original laboratory sample of “M and B 693” or sulphapyridine, small quantity of yellowish white powder produced by May and Baker of Dagenham, bottle inserted in black wooden mount, English, 1930-1938
M & B 693 was one of the first generation of sulphonamide antibiotics, pro-duced for the first time in 1938. The first chemical cure for pneumonia, it was hailed as a wonder drug. M & B 693 could also prevent the growth of the blood-poisoning bacteria in wounds and was used to protect against gan-grene. It could either be taken in tablet form or the powder could be placed in wounds. It was used so widely during the Second World War that May & Baker had difficulty keeping up with demand. It was later largely superseded by penicillin and sulphonamides.
Above: Dysentery patient 1943 Burma. (we acknowledge and thank IWM)
Above: A Confronting photo of POWs of ‘F’ Force with dysentery on their train trip from Singapore to Thailand 1943. It was similar for every POW entrained to Thailand to work.
Above: We wish to acknowledge IWM for above dipiction of a dysentery ward.
Did you know dysentery has played significant roles in Australian military history?
Epidemic dysentery occurred on the Gallipoli Peninsula in 1915 – soldiers were crowded into unhygienic situations for days at a time, there was no water and the rocky soil prevented normal latrine construction. It was a factor in consideration to leave the peninsula.
In Palestine 1918, Australians suffered dysentery in the hot Jordan Valley.
Twenty per cent of autopsies performed at No. 3 Australia General Hospital in Egypt WW1 showed amoeba. Most deaths were either acute infections driven by the Shiga bacterial toxin or chronic infections resulting in malnutrition and debilitation.
WW2 in New Guinea was a prime area for dysentery as well as Queensland and N.T.
There was an outbreak of dysentery for some of the Australian soldiers in Vietnam.
Dysentery through History
During the 1700s and 1800s dysentery disease caused endless deaths throughout Europe.
Diarrheal diseases are among the most common causes of death, especially in children in developing countries. In 2019 around 1.5 million people died from diarrheal diseases.
Malaria on Burma- Thai Railway
In his memoirs, Stanley P. Pavillard, a POW medical officer in the No.4 Camp, states that
“The worst of the acute and dangerous diseases which we were faced with, apart from cholera, was malignant tertian malaria with its cerebral complications.”
Almost everyone on the railway contracted malaria: in memoirs of ex-POWs and former Japanese servicemen, malaria is always mentioned as a disease that the authors suffered from. In most cases, the disease was ʻbenign tertianʼ malaria caused by Plasmodium vivax. However, according to Gill, in remote camps in the jungle, up to one-third of cases were falciparum malaria caused by Plasmodium falciparum, which was malignant and associated with complications, including cerebral malaria.
Pavillard described cerebral malaria patients as follows:
“Patients were being brought in with temperatures of 105°to 107°, and unless the proper diagnosis was made and the proper treatment given at once, the patient would sink into delirium and then into a coma, and his temperature would rise to 110°: after this there was no hope of recovery as his brain was literally cooked. The important thing therefore was to keep the temperature down.”
Pavillard would then slowly inject quinine well diluted in saline into the patients’ veins, although it could lead to sudden heart failure. It was the only life-saving technique they had. Quinine is usually used to treat uncomplicated malaria, not severe forms of the disease. Nevertheless, the only medicine that the IJA could provide to treat malaria was quinine, and a sufficient amount was available.
In his report, Tagami states that: Even the Japanese forces in this [Thai-Burma border] area, when outbreaks of malaria occurred, would have been without the ability to carry out operations but for the fact that we had a considerable stock of quinine.
Thus, the POWs could obtain the medicine sufficiently. Also POW medical officers could get more quinine from the Japanese by padding the number of malaria patients. For instance, Hardie, a medical officer in the No.2 Camp, states in a note for his diary that, at first, in view of the inadequacy of the supply of quinine, he was compelled to inflate the number of malaria patients. However, in the entry on 7 July 1943, Hardie states that they were getting enough quinine to treat active cases.
Pavillard also padded the number of malaria patients and obtained more quinine than he needed. Eventually, the ʻemergency reserveʼ of quinine was exchanged with a cow owned by a local Thai resident.
Pavillard adds that “It was impossible to cope with malaria and its complications properly.” Besides the insufficiency of malaria preventive measures, there was a problem among the POWs. Even after a sufficient amount of quinine became available, many POWs refused to take the medicine either for prevention or cure. Pavillard often found the pills, supposed to have taken, hidden under their pillows after they had died. Presumably, the POWs refused the medication for its adverse effects. Therefore, prevention became still more essential. Accordingly, mosquito-nets and blankets became precious items, and thefts became frequent in the POW camps. Baynes recollects in his memoirs as follows:
There was unfortunately a lot of thieving from comrades going on in Chunkai camp. […] Blankets, most valuable of all the captiveʼs possessions, were stolen and sold to the Thais. With no protection from the malaria-carrying mosquito many must have died solely because of these camp thieves. Even the medical hut was broken into and our scanty supply of medicines robbed for private gain. Some became so wealthy that they were able to bribe those in charge to let them stay in camp as sick men, while the really sick were forced out to work.
There was friction among officer POWs in the No.2 Camp regarding anti-malaria activities such as oiling mosquitoes’ breeding grounds. When Hardie formed an anti-malaria working party comprised of officers, some officers worked hard, but others were reluctant, saying that officers should not do the work. Moreover, in his diary, Hardie criticises Williamson, the No.2 Camp Commander, for his uncooperative attitude towards the anti malaria party. Hardie said that:
apparently the Japs are trying to get more officers out working on the railway and it looks as if Colonel Williamson, anxious as ever to comply, was trying to put the blame on me for the necessity of turning the anti-malaria party officers on to railway work.
So, not only mosquitos but also enemies and comrades were the factors that made malaria prevalent among the POWs!
We wish to ackowledge the above Malaria information has been taken from
Constructing the Burma-Thailand Railway: The War Crimes Trials and the Shaping of an Episode of WWII – by Kazunori Hashimoto. Thesis submitted for the degree of PhD YEAR 2022
Markowitz was born 1901 Husi and lived most of younger years in Bucharest, Romania. He attended Jarvis Collegiate and later attended the University of Toronto, where he obtained his medical degree and a doctorate in 1926 in Physiology. He was appointed Assistant Professor in Physiology at Glasgow University 1926-27. and later Professor of Physiology at Georgetown University, USA 1930-1932. Markowitz became an expert in the field of intricate organ surgery, and the first person in the world to transplant the heart of one warmblooded animal into another in 1932. His knowledge, expertise and skill would help him save hundreds of POW lives.
In 1941, Jacob Markowitz went to England, where he joined the Royal Army Medical Corps as a captain. Sent to Singapore he supported the Indian Medical Services and was posted to 5 Casualty Clearing Station during the fighting in Malaya. He was taken POW of Japan when the surrender occurred 15 February 1942. He was moved into the British Barracks.
On the Burma-Thai Railway Markowitz was highly regarded. He stood out as being highly intelligent and astute, was always optimistic, sharp and bright and as a Professor of Physiology stood out academically. During his time at Chungkai and Nakom Pathom Markowitz performed over 1,000 operations (including more than 100 amputations of the thigh for tropical ulcers) and 3,800 transfusions (25 on one Australian patient).
He relied on dedicated assistants improvise and make medical instruments and transfusion units, etc. He developed the transfusion of defibrinated blood at these two camps in Thailand.
Markowitz was highly regarded. He stood out as being highly intelligent and astute, was always optimistic, sharp and bright and as a Professor of Physiology stood out academically. During his time at Chungkai and Nakom Pathom Markowitz performed over 1,000 operations (including more than 100 amputations of the thigh for tropical ulcers) and 3,800 transfusions (25 on one Australian patient).
He relied on his three medical assistants to improvise and make medical instruments and transfusion units, etc. He developed the transfusion of defibrinated blood at these two camps in Thailand.
Above: Markowitz with his backs toward the artist undertaking an amputation.
Markowitz said after the war:
“The Japanese guards fed sick prisoners pig-feed but even pigs could not live on it. It is because of starvation chiefly that to have been a prisoner of war of the Japanese army in 1942-43 involved, actuarially speaking, a greater risk than [that] faced by a fighter pilot in the Battle of Britain or by an army of Canadians bravely fighting their way through Holland.”
After the war Dr. Markowitz was awarded one the highest of British military honours: the Order of the British Empire. The citation read:
“As joint originator and supervisor of a fully successful transfusion service in prisoner of war camps in Siam using the most primitive and improvised apparatus, Captain Markowitz has shown skill and ability of an outstanding degree. His training of transfusion teams, his development of simple techniques for jungle surgery and his ingenious methods of improvisation saved many hundreds of lives. He has shown great disregard for personal danger and risk of brutality in order to serve his patients.”
The main causes of POW deaths were maltreatment, starvation, overwork and disease. The work itself was very often gruelling, and dangerous. They worked excessively long hours whilst sick, without medicines with very, very little food and at times no rest days. They were subjected to unexpected brutality.
WX9004 Albert Cryer was evacuated with a large number of sick from ‘D’ Force S Battalion working on Burma-Thai Railway Hellfire pass region to Kanu 1 River Camp – which was not a camp with shelter, it was a staging post for the sick to barge south down the river to POW hospital camps. It was while waiting to board a barge that very ill Albert Cryer died of typhus on 28 July 1943 aged 32 years.
Above: Albie Cryer
While at 75 Kilo camp, and working as solo doctor, Albert Coates, Head Surgeon of AIF was incapacitated with scrub-typhus and many of the men thought he would die. Although he could not stand, the Japanese sent him to run a new hospital camp 55 kilo at Kohn Kuhn where the main body of sick and injured would be taken. Coates was so sick, he had to be carried around the camp site while construction was completed and he examined the sick. He was forever grateful to two men who looked after him during his illness, Harold Buckley, who was suffering from malaria himself, and a Dutchman, Capt C J Van Bentinck who also provided great care.’
Coates, Albert
Other members of ‘D’ Force S Battalion to die of Typhus included:
WX8639 Joseph John (JJ) LYNCH, ‘D’ Force S Btn died cholera and typhus at Kanu 1 River Camp 1 Aug 1943 aged 34 years. Just a few days after Albert Cryer. He had been evacuated with large number sick POWs and was waiting for a barge to be transported.
WX8820 Wallace Patrick MCCUDDEN from Esperance was evacuated from Burma-Thai Railway and died at Chungkai Hospital Camp 21 Aug 1943 of cardiac beri beri and Typhus aged 36 years.
SCRUB TYPHUS is a very serious disease.
Scrub typhus is a disease caused by bacteria called Orientia tsutsugamushi, which is in the rickettsia family.
How it is spread
The bacteria infect people when they are bitten (usually painlessly) by an infected larval mite called
Leptotrombidium deliense. The mite is very small (0.2 to 0.4mm) and can often only be seen through a microscope or magnifying glass.
The mites live in grassland areas at the edge of dense monsoon forests or forested creeks. Mites usually feed
on marsupials and other native animals such as rats but they can attach to passing humans and bite for a blood meal.
Scrub typhus cannot spread from one person to another.
Symptoms
The symptoms usually occur within 1 to 2 weeks of being bitten. They may include fever, chills, sweating,
headache, muscle aches, swollen glands, nausea/vomiting and a skin rash. The bite site often ulcerates and becomes red with a central black scab, called an “eschar”. The bite site may be on the buttocks or genitalia, including when people have been bitten while sitting, and in the armpit.
Where is the disease found
Scrub typhus is found in the Asia-Pacific region including northern Australia. The endemic area extends from. south-eastern Siberia and northern Japan, through eastern and south-east Asia, to Vanuatu in the east and Pakistan in the west. Other countries may have small foci. North Thailand has the highest prevalence of disease.
There have been numerous reported cases of infection in the Top End of the Northern Territory since 1990.
We wish to acknowledge much of the above information is taken from NT Health Fact Sheet.
Today, April 2024 Scrub Typhus continues to exist in Asian countries, in particular Northern Thailand. Research reveals Scrub Typhus responds to only a few specific antibiotics, the main one being doxycycline which has been around for a few decades.
If you develop fever within the endemic area (northern Thailand) and go to hospital you are most likely to receive another class of antibiotics similar to penicillin which have no action against scrub typhus.
In northern Thailand the scrub typhus mortality can be as high as 13%, which is quite high. This region accounts for 50-60% of these cases, despite only containing 20% of the population.
From Moru – Tropical Health Network
‘Scrub typhus is a neglected tropical disease, so neglected in fact that the World Health Organisation does not have scrub typhus listed as one of the official neglected tropical diseases. As a disease that’s been under-researched and underfunded for decades, we are light years away from being in the position of other major diseases such as HIV, TB and malaria. The fact that drug resistance has been reported, and the fact that there are no effective vaccines currently available.’
Armed with this information it is not difficult to believe Albie Cryer and JJ Lynch had only a small chance of survival – and without any treatment and waiting for a barge in the open (Kanu staging camp was not a camp, that is, no roof or structure) his health would have deteriorated rapidly.
BLACKWATER FEVER -just another tropical illness for POWs!
We are positive Australian and British doctors on the Line had never previously heard of Blackwater fever, let alone the means to treat it.
Blackwater fever is a severe clinical syndrome occurring as a complication of malaria in other words Blackwater fever is a type of rare and complicated malaria infection.
Symptons include a rapid pulse, high fever/chills, vomiting, blood in urine, increased heart rate, jaundice. The person will experience fatigue and too much weakness, a rapidly developing anemia, and the passage of urine that is black or dark red in colour (hence the disease’s name).
In some cases the skin may become dry, thin and scaly in patches and hair may be lost. In people with a light skin tone, greyish discolouration of the skin of hands, feet, abdomen and face may be seen, that is why the disease is also called black fever.
Without proper diagnosis and treatment, blackwater fever is associated with high fatality.
DR PETER HENDRY, MO 2/10TH AUSTRALIAN FIELD AMBULANCE – ‘F’ FORCE
We wish to acknowledge author Pattie Wright and her book ‘THE MEN OF THE LINE’ and her interview with Hendry.
Hendry was one of several young doctors sent with ‘F’ Force Thailand. As a 26 year old he found himself in a foreign country in circumstances he could never ever have envisaged and treating diseases he would have only read about if he was fortunate.
Hendrys obituary: Peter studied Medicine at Sydney University. At first, inspired by his father’s example he wanted to be a ‘medical missionary’ but over time that changed into Surgery and ultimately into Pathology. That was the right decision for him and certainly the best decision for Pathology.
He worked at Neikhe, Lower Sonkurai and Sonkurai where he remained for the longest time, six months. Hendry was fortunate never to contract malaria.
Neikhe – Hendry’s job was mostly to pick the men from the line of sick POWs to be sent out to work. A most trauma filled responsibility. Hendry felt the sick hated him and each one hoped he would not be sent. Hendry admitted he didn’t stand up to the Japs – but those who did were bashed and the Japs always got the number of men they wanted.
Sonkurai – building a big bridge across the river
The British had been here for three months and were in terrible shape. The Senior Officer Lt Colonel FJ Dillon (later Brigadier), a regular soldier in the British Army, a magnificent man, revered by all who survived. Songkurai was reputably the worst camp of them all; its Death Toll was the highest. There was no proper hygiene, no control and the camp was in crisis. Hendry wrote, the powers that be (I imagine he is referring the British leadership) set Hendry up with 2 atap huts in their own area away from the main camp – the British hospital with 800 patients which were being cared for by Australian doctors Lloyd Cahill and John Taylor.
Hendry was in charge of the patients who were too sick to work and really came to die. There was always between 50 and 100 patients. Hendry talks about his group of 10 orderlies – who were given the name ‘Universal Providers.’
Hendry had with him Ted McGlynn, Harry Williams, Reg Jarman, Bob Wilson and a number of highly experienced 12/10 Field Ambulance staff who were referred to as ‘Scroungers’ because they could ‘find’ most things required. Hendry told Don Wall for ‘Heroes of ‘F’ Force’ he found the British medical orderlies were senior to some of his top men who were Privates, so he promoted them unknown to the British, so they then became senior. Hendry believes Lt. Col Dillon the Senior British officer, would have been aware of the promotion but said nothing. He had used some of these resourceful Australians to purchase goods from the Thai traders without the Japanese knowing.
‘The hospital became a happier place with the Australians entirely involved in running the camp. Capt Hendry livened up the camp hospital with a few concerts – “Benjo Pete and his Poopsters’ singing western songs!’
Hendry put in charge of cleaning up the camp one of his orderlies Pte Harry Williams who did a wonderful job. Gave orders to the Poms and took responsibility for the Camp.
The group of 10 young soldiers came from around Casino, NSW – country hicks. Initially lost when they first joined AIF, the young men stayed together through the entire war, even on the Line. The ‘Universal Providers’ earned their name because they would go under the wire and buy anything. Three of them would die on the Line, one at Sokurai.
Fortunately the Japs were too terrified and did not come near them because it was a death camp for the very ill and dying POWs. There was not a POW who could work! Hendry and his hard-working orderlies tried their best to keep their patients cheerful, comfortable and mobile if they could. They medical staff presented two concerts for the patients.
Hendry considered beri beri the worst illness. Once you had beri beri then a POW was susceptible to malaria and cholera. They had no medical supplies to deal with cholera.
While Peter Hendry was at Songkurai Capt Lloyd Cahill was left in charge at Lower Sonkurai to supervise the evacuation and transfer of those men allocated to Sonkurai and Upper Sonkurai. This move effectively split Units and the highly successful junior officers who carried the administration of the camp were now surplus to the less efficient officers.
Hendry wrote his youthful enthusiasm got him through this time on the line, however he was delighted to return to the ‘land of milk and honey’ – Changi.
Hendry was positive Sonkurai was the very worst camp on the Line. Certainly there were some notoriously cruel and sadistic Japanese at Sonkurai.
Above: Doctors Cahill, Vic Brand & Hendry at Singapore
His was an extraordinary life. Peter Hendry died aged 102 years NSW.

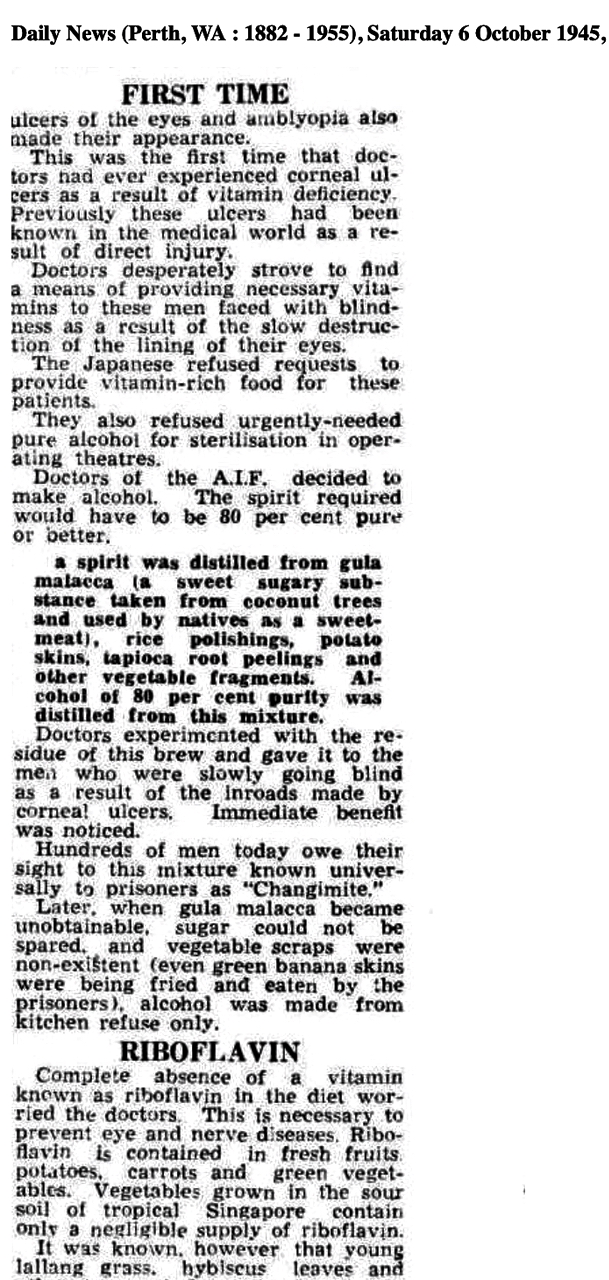
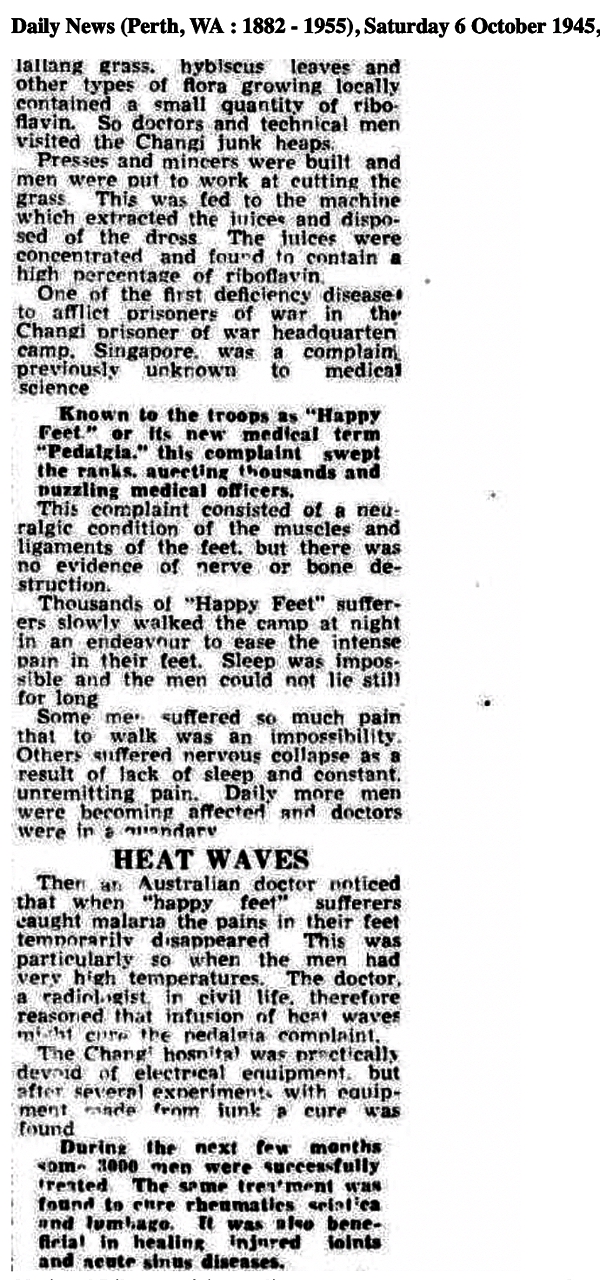
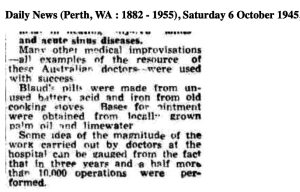




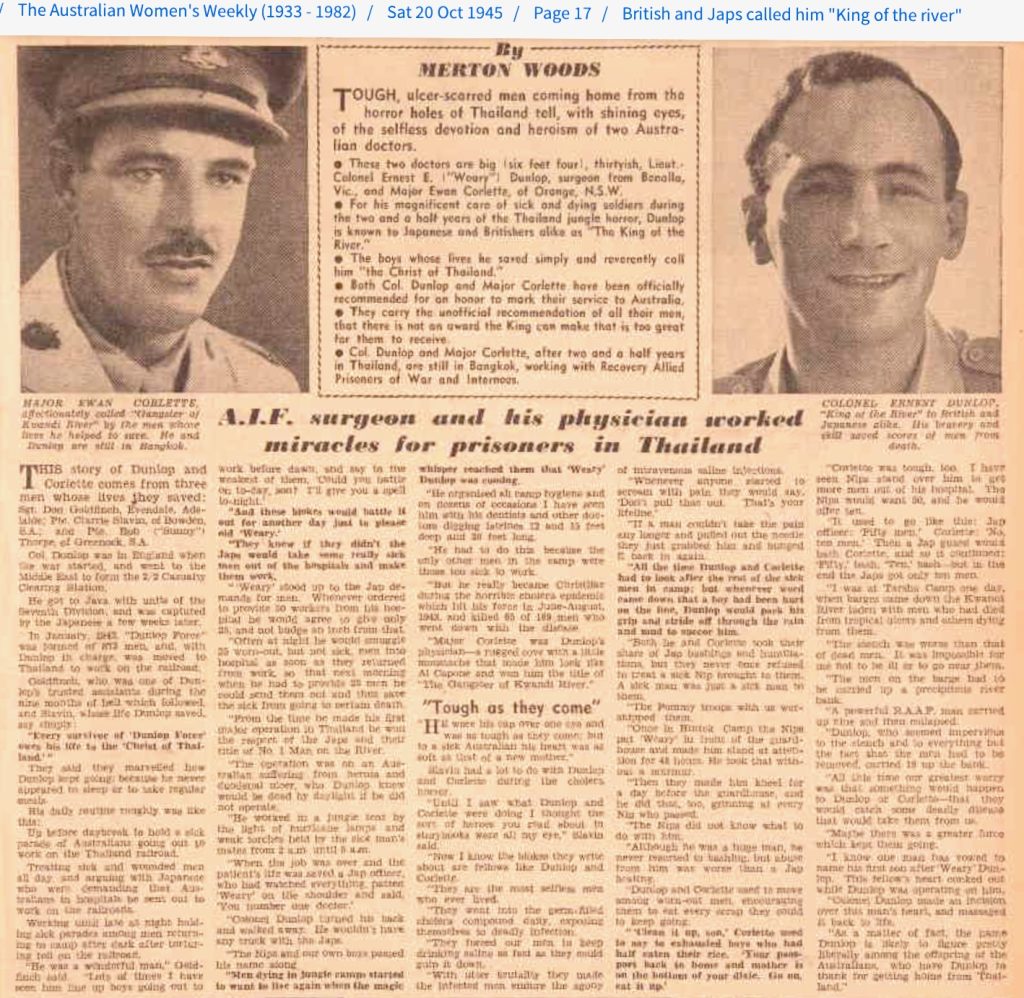
 John Chalmers was born in Sydney on 20 March 1910. He went to high school at Fort Street Boys High School and studied medicine at Sydney University. He also served in the Militia as a member of Sydney University Regiment for a number of years.
John Chalmers was born in Sydney on 20 March 1910. He went to high school at Fort Street Boys High School and studied medicine at Sydney University. He also served in the Militia as a member of Sydney University Regiment for a number of years.